Mo Shaobo, Wang Hui, Han Lingyu, Xiang Wenqiang, Dai Weixing, Zhao Pengfei, Pei Fengchun, Su Zhixi, Ma Chengcheng, Li Qi, Wang Zhimin, Cai Sanjun, Wang Hao, Liu Rui, Cai Guoxiang
Department of Colorectal Surgery, Fudan University Shanghai Cancer Center, Shanghai, China.
Department of Oncology, Shanghai Medical College, Fudan University, Shanghai, China.
Front Oncol. 2021 Feb 25;11:643136. doi: 10.3389/fonc.2021.643136. eCollection 2021.
Fecal immunochemical test (FIT), DNA mutation, DNA methylation, and microbial dysbiosis all showed promising in colorectal cancer (CRC) non-invasive detection. We assessed CRC detection with an assay combining all these strategies and investigated the effect of clinical features on the performance of this comprehensive test.
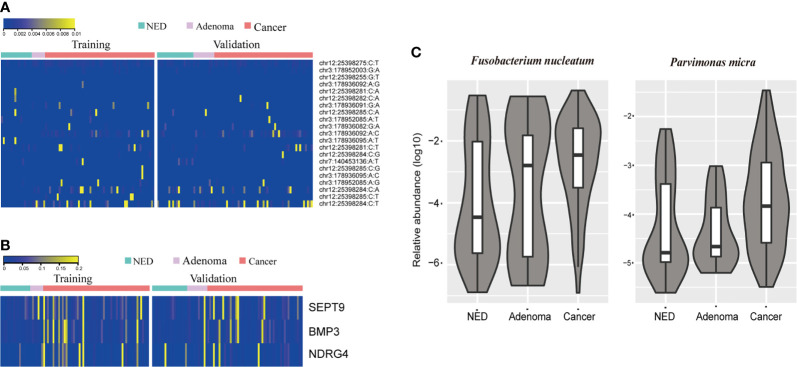
We performed a multidimensional analysis study using stool samples collected from 108 patients with CRC, 18 patients with colorectal adenoma, and 36 individuals with no evidence of colorectal disease. The multidimensional analysis of stool samples including FIT, stool DNA (sDNA) tests for three methylated genes (Septin9, NDRG4, BMP3) and three mutated genes (KRAS, BRAF, PI3KCA) using next generation sequencing as well as detection of stool bacteria level of and using qPCR method. We used a linear support vector classification model to analyze the data.
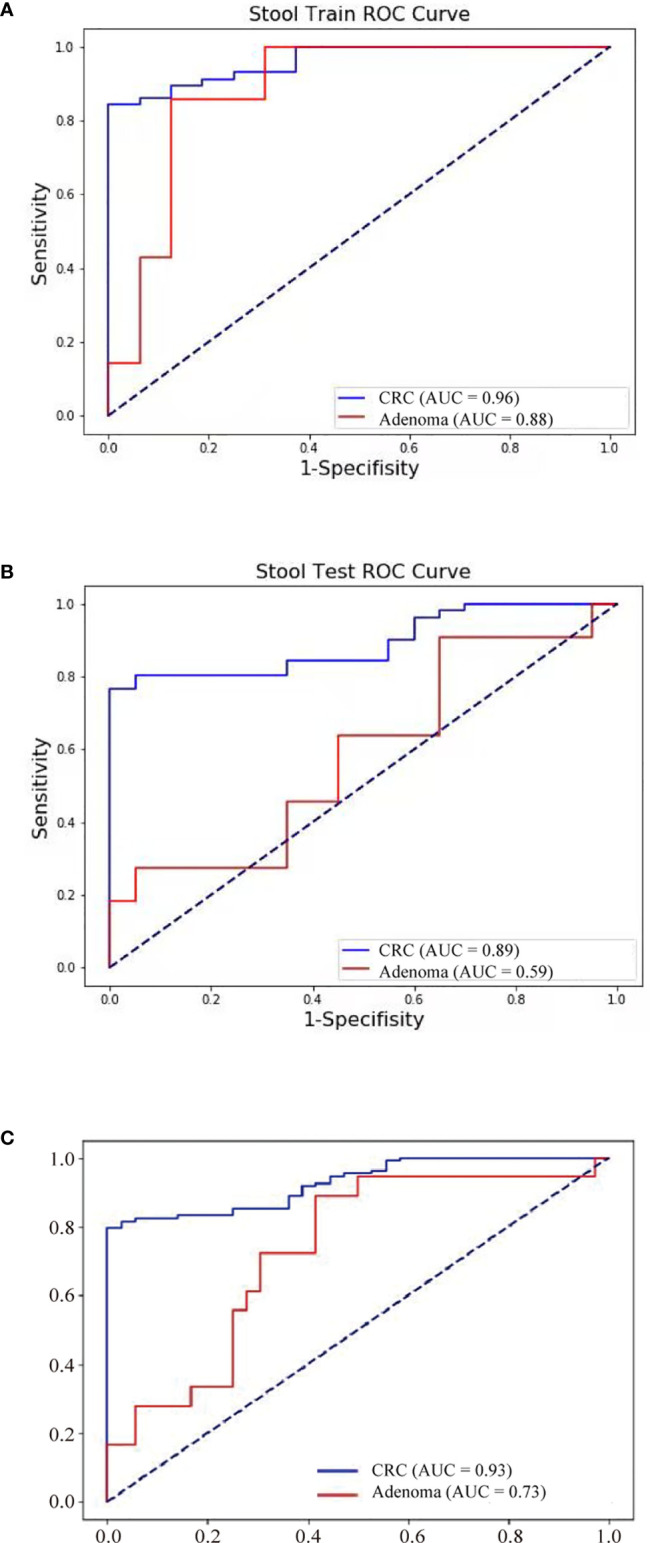
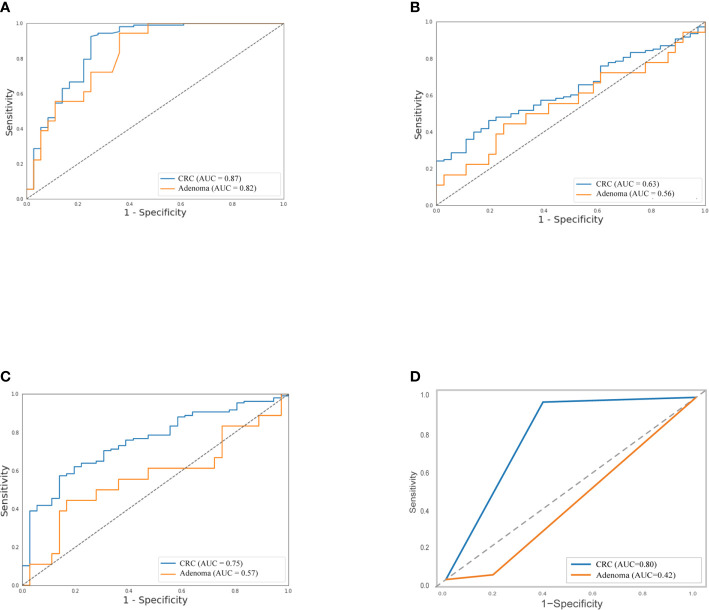
The sensitivity of FIT alone was 69.4% for CRC and 11.1% for adenoma. Separately, the sensitivity of the detection of intestinal bacteria, DNA mutation, and DNA methylation for CRC was 58.3, 50.0, and 51.9%, respectively. The combination of FIT and sDNA tests had a sensitivity of 81.5% for CRC (AUC: 0.93, better than FIT alone, P = 0.017) and 27.8% for adenoma with 94.4% specificity. Sensitivity of the multidimensional test to detect CRC with stage II (84.6%) and III (91.9%) CRC was relatively higher (88.2%) than that of patients with stage I (60.0%) and stage IV (75.0%) (P = 0.024). The rate of CRC detection increased with tumor size (P = 0.008) and age (P = 0.04). Interestingly, the rate of CRC detection was higher in smoking persons than non-smokers with marginal significance (P = 0.08).
The multidimensional assay of stool samples combining FIT and stool DNA tests further improved the diagnostic sensitivity for CRC. This could provide new approach for improvement of CRC screening and further demonstrations are warranted.
粪便免疫化学检测(FIT)、DNA突变、DNA甲基化和微生物群落失调在结直肠癌(CRC)的非侵入性检测中均显示出良好前景。我们评估了一种结合所有这些策略的检测方法对CRC的检测效果,并研究了临床特征对这种综合检测性能的影响。
我们使用从108例CRC患者、18例结直肠腺瘤患者和36例无结直肠疾病证据的个体中收集的粪便样本进行了一项多维分析研究。对粪便样本进行多维分析,包括FIT、对三个甲基化基因(Septin9、NDRG4、BMP3)和三个突变基因(KRAS、BRAF、PI3KCA)进行粪便DNA(sDNA)检测(采用下一代测序技术)以及使用qPCR方法检测粪便细菌水平。我们使用线性支持向量分类模型分析数据。
单独FIT对CRC的敏感性为69.4%,对腺瘤的敏感性为11.1%。单独来看,肠道细菌检测、DNA突变检测和DNA甲基化检测对CRC的敏感性分别为58.3%、50.0%和51.9%。FIT和sDNA检测相结合对CRC的敏感性为81.5%(曲线下面积:0.93,优于单独的FIT,P = 0.017),对腺瘤的敏感性为27.8%,特异性为94.4%。多维检测对II期(84.6%)和III期(91.9%)CRC的检测敏感性相对高于I期(60.0%)和IV期(75.0%)的患者(P = 0.024)。CRC检测率随肿瘤大小(P = 0.008)和年龄(P = 0.04)增加。有趣的是,吸烟者的CRC检测率高于非吸烟者,差异具有边际显著性(P = 0.08)。
结合FIT和粪便DNA检测的粪便样本多维检测进一步提高了CRC的诊断敏感性。这可为改进CRC筛查提供新方法,值得进一步论证。