López-Vilella Raquel, Marqués-Sulé Elena, Laymito Quispe Rocío Del Pilar, Sánchez-Lázaro Ignacio, Donoso Trenado Víctor, Martínez Dolz Luis, Almenar Bonet Luis
Heart Failure and Transplant Unit, La Fe University and Polytechnic Hospital, Valencia, Spain.
Cardiology Department, La Fe University and Polytechnic Hospital, Valencia, Spain.
Front Cardiovasc Med. 2021 Mar 5;8:618398. doi: 10.3389/fcvm.2021.618398. eCollection 2021.
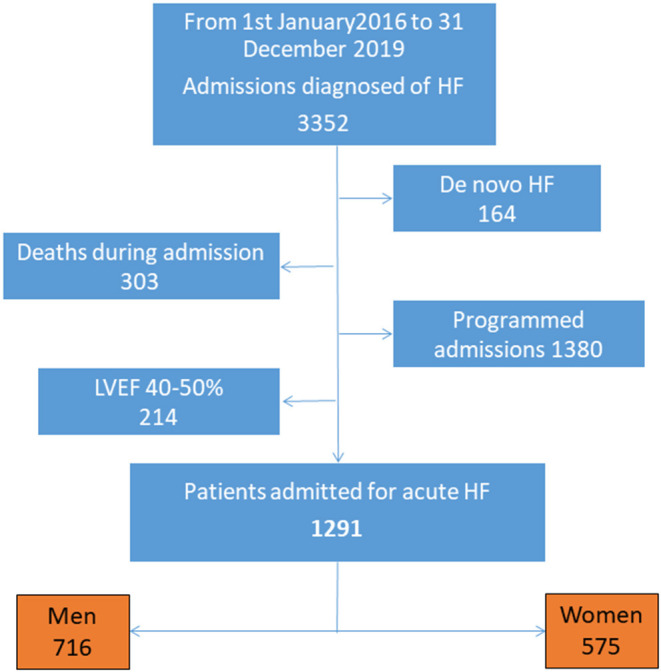
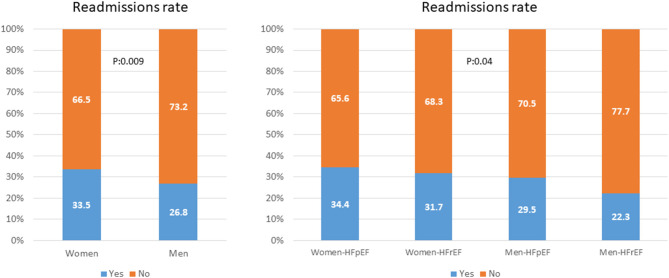
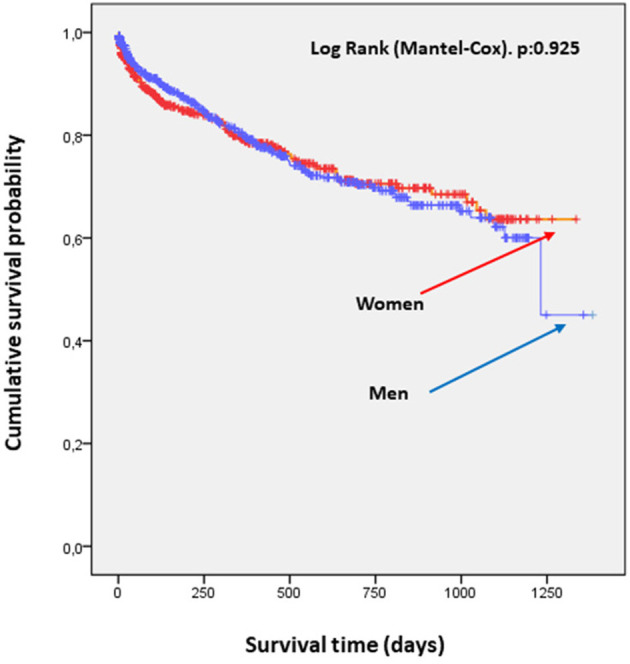
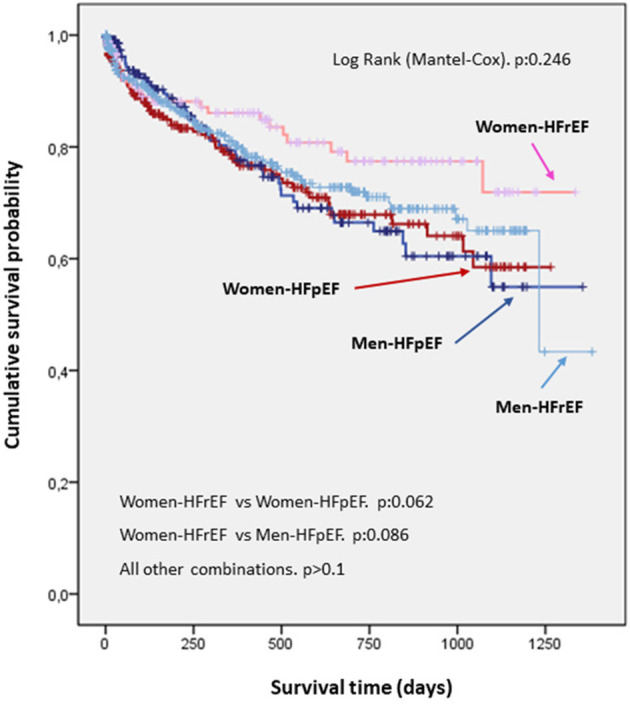
Heart failure (HF) is a major cause of morbimortality both in men and women. Differences between sex in etiopathogenesis, response to treatment, and quality of care have been found in patients with HF. Females are usually under-represented in clinical trials and there is no solid evidence demonstrating the influence of sex in the prognostic of chronic HF. The primary objective of this study was to analyse the differences in mortality and probability of hospital readmission between males and females with HF. The secondary objective was to compare mortality and probability of hospital readmission by ejection fraction (reduced vs. preserved). Patients with decompensated HF that were consecutively admitted to a Cardiology Service of a tertiary hospital for 4 years were recruited. HF, death during hospitalization, programmed admissions and those patients with moderate left ventricular ejection fraction (LVEF) (40-50%) were discarded. Finally, 1,291 patients were included. Clinical profiles, clinical history, functional status, treatment at admission, first blood analysis performed, readmissions and mortality at follow-up were analyzed and compared. All patients underwent an echocardiographic study at admission. HF with reduced ejection fraction (HFrEF) was considered when left ventricular ejection fraction (LVEF) was <40%, whilst HF with preserved ejection fraction (HFpEF) was considered when LVEF was ≥50%. 716 participants were male (55%). Basal characteristics showed differences in some outcomes. No differences were found in probability of survival among patients with decompensated HF by sex and ejection fraction ( = 0.25), whereas there was a clear tend to a major survival in females with HFrEF ( < 0.1). Females presented more readmissions when compared to males, independently from the LVEF (females = 33.5% vs. males = 26.8%; = 0.009). Adjusted multivariate analysis showed no association between sex and mortality (HR = 0.97, IC 95% = 0.73-1.30, = 0.86), although there was association between female sex and probability of readmission (OR = 1.37, IC 95% = 1.04-1.82, = 0.02). Sex does not influence mid-term mortality in patients admitted for decompensated HF. Nevertheless, probability of readmission is higher in females independently from LVEF. Thus, it should be considered whether healthcare may be different depending on sex, and a more personalized and frequent care may be recommended in females.
心力衰竭(HF)是男性和女性发病和死亡的主要原因。在心力衰竭患者中,已发现性别在病因发病机制、对治疗的反应和护理质量方面存在差异。女性在临床试验中的代表性通常不足,并且没有确凿证据表明性别对慢性心力衰竭的预后有影响。本研究的主要目的是分析男性和女性心力衰竭患者在死亡率和再次入院概率方面的差异。次要目的是比较射血分数(降低与保留)的死亡率和再次入院概率。招募了连续4年因失代偿性心力衰竭入住三级医院心脏病科的患者。排除心力衰竭、住院期间死亡、计划性入院以及中度左心室射血分数(LVEF)(40-50%)的患者。最终纳入1291例患者。对临床特征、临床病史、功能状态、入院时的治疗、首次血液分析、随访时的再次入院和死亡率进行了分析和比较。所有患者入院时均接受了超声心动图检查。当左心室射血分数(LVEF)<40%时,考虑为射血分数降低的心力衰竭(HFrEF),而当LVEF≥50%时,考虑为射血分数保留的心力衰竭(HFpEF)。716名参与者为男性(55%)。基础特征在一些结果上显示出差异。失代偿性心力衰竭患者按性别和射血分数分类的生存概率无差异(P = 0.25),而HFrEF女性患者有明显更高的生存倾向(P < 0.1)。与男性相比,女性再次入院的情况更多,与LVEF无关(女性 = 33.5% 对男性 = 26.8%;P = 0.009)。调整后的多变量分析显示性别与死亡率之间无关联(HR = 0.97,95%CI = 0.73-1.30,P = 0.86),尽管女性性别与再次入院概率之间存在关联(OR = 1.37,95%CI = 1.04-1.82,P = 0.02)。性别不影响因失代偿性心力衰竭入院患者的中期死亡率。然而,无论LVEF如何,女性再次入院的概率更高。因此,应考虑医疗保健是否可能因性别而异,并可能建议对女性进行更个性化和更频繁的护理。