Clinical Enteric NeuroscienceTranslational and Epidemiological Research (CENTER), Division of Gastroenterology and Hepatology, Mayo Clinic, Rochester, Minnesota.
Department of Laboratory Medicine and Pathology, Mayo Clinic, Rochester, Minnesota.
Gastroenterology. 2021 Aug;161(2):463-475.e13. doi: 10.1053/j.gastro.2021.04.020. Epub 2021 Apr 16.
Oral monosaccharides and disaccharides are used to measure in vivo human gut permeability through urinary excretion.
The aims were as follows: (1) to obtain normative data on small intestinal and colonic permeability; (2) to assess variance on standard 16 g fiber diet performed twice; (3) to determine whether dietary fiber influences gut permeability measurements; and (4) to present pilot data using 2 selected probes in patients with diarrhea-predominant irritable bowel syndrome (IBS-D).
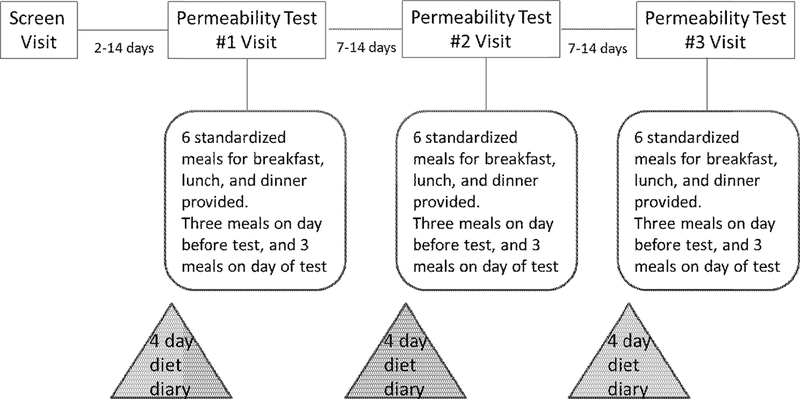
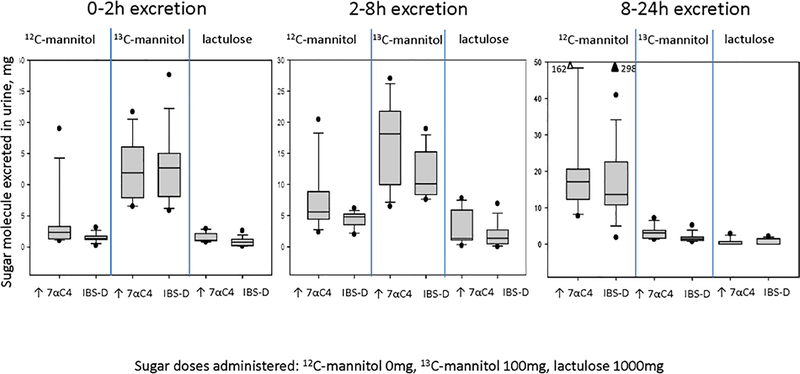
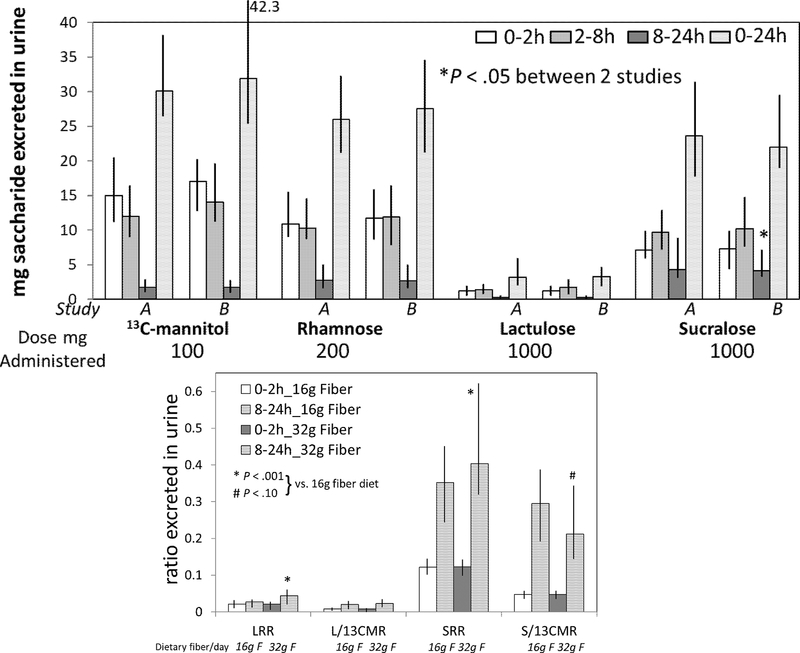
Sixty healthy female and male adults, age 18-70 years, participated in 3 randomized studies (2 studies on 16.25 g and 1 study on 32.5 g fiber) in otherwise standardized diets. At each test, the following sugars were ingested: C-mannitol, C-mannitol, rhamnose (monosaccharides), sucralose, and lactulose (disaccharides). Standardized meals were administered from 24 hours before and during 24 hours post-sugars with 3 urine collections: 0-2, 2-8, and 8-24 hours. Sugars were measured using high-performance liquid chromatography-tandem mass spectrometry. Eighteen patients with IBS-D underwent 24-hour excretion studies after oral C-mannitol and lactulose.
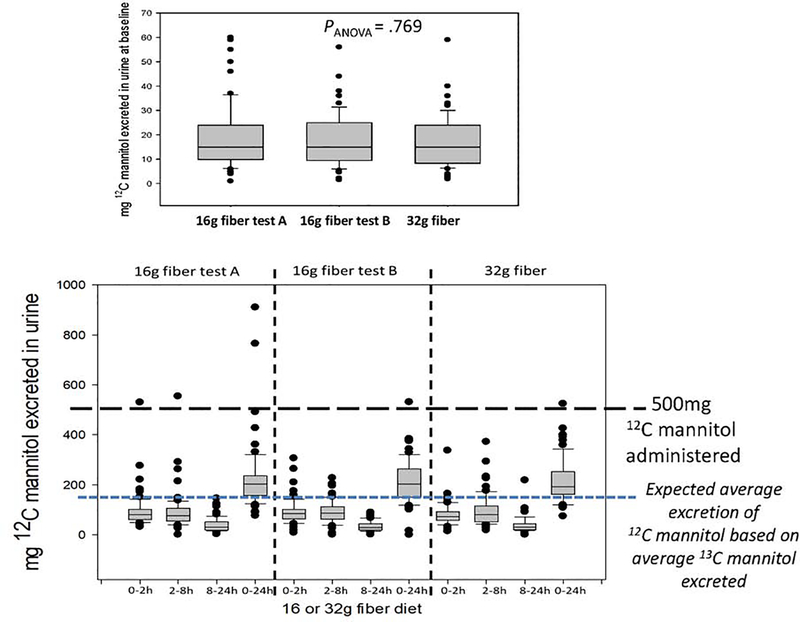
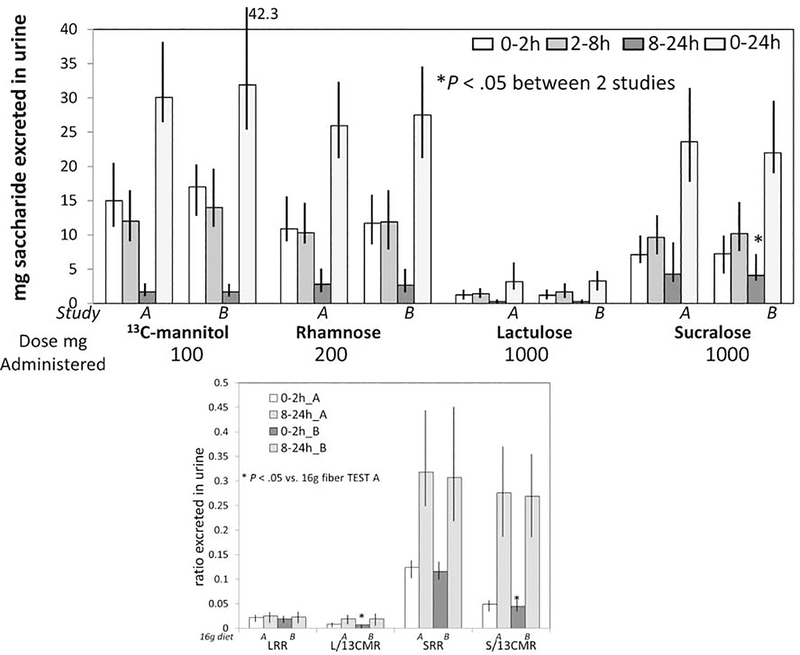
Baseline sugars (>3-fold above lower limits of quantitation) were identified in the 3 studies: C-mannitol in all participants; sucralose in 4-8, and rhamnose in 1-3. Median excretions/24 h (percentage of administered dose) for C-mannitol, rhamnose, lactulose, and sucralose were ∼30%, ∼15%, 0.32%, and 2.3%, respectively. C-mannitol and rhamnose reflected mainly small intestinal permeability. Intraindividual saccharide excretions were consistent, with minor differences with 16.25 g vs 32.5 g fiber diets. Median interindividual coefficient of variation was 76.5% (10-90 percentile: 34.6-111.0). There were no significant effects of sex, age, or body mass index on permeability measurements in health. C-mannitol measurements are feasible in IBS-D.
Baseline C-mannitol excretion precludes its use; C-mannitol is the preferred probe for small intestinal permeability.
口服单糖和二糖被用于通过尿液排泄来测量体内人类肠道通透性。
本研究的目的如下:(1)获得小肠和结肠通透性的正常数据;(2)评估两次标准 16 克纤维饮食的差异;(3)确定膳食纤维是否会影响肠道通透性的测量;(4)在腹泻型肠易激综合征(IBS-D)患者中使用 2 种选定的探针提供初步数据。
60 名年龄在 18-70 岁的健康女性和男性成年人参加了 3 项随机研究(2 项研究使用 16.25 克纤维,1 项研究使用 32.5 克纤维),均在标准饮食下进行。在每次试验中,均摄入以下糖:C-甘露醇、C-甘露醇、鼠李糖(单糖)、蔗糖素和乳果糖(二糖)。在摄入糖前 24 小时至摄入后 24 小时内给予标准化餐,共采集 3 次尿液:0-2、2-8 和 8-24 小时。使用高效液相色谱-串联质谱法测量糖。18 名 IBS-D 患者在口服 C-甘露醇和乳果糖后进行了 24 小时排泄研究。
在 3 项研究中均发现基线糖(高于定量下限的 3 倍以上):所有参与者均有 C-甘露醇;4-8 项有蔗糖素,1-3 项有鼠李糖。C-甘露醇、鼠李糖、乳果糖和蔗糖素的 24 小时排泄量/(给予剂量的百分比)分别约为 30%、15%、0.32%和 2.3%。C-甘露醇和鼠李糖主要反映小肠通透性。个体内糖的排泄是一致的,16.25 克纤维饮食与 32.5 克纤维饮食之间仅有微小差异。个体间变异系数的中位数为 76.5%(10-90%分位数:34.6-111.0)。在健康人群中,性别、年龄或体重指数对通透性测量无显著影响。C-甘露醇测量在 IBS-D 中是可行的。
基线 C-甘露醇排泄排除了其用途;C-甘露醇是测量小肠通透性的首选探针。