Wallis T J M, Heiden E, Horno J, Welham B, Burke H, Freeman A, Dexter L, Fazleen A, Kong A, McQuitty C, Watson M, Poole S, Brendish N J, Clark T W, Wilkinson T M A, Jones M G, Marshall B G
Department of Respiratory Medicine and Southampton NIHR Biomedical Research Centre, University Hospital Southampton and School of Clinical and Experimental Sciences, Faculty of Medicine, University of Southampton, Southampton, UK.
NIHR Southampton Biomedical Research Centre Research Fellow, University of Southampton, MP218 D-Level South Academic Block University Hospital Southampton, Southampton, SO16 6YD, UK.
Respir Res. 2021 May 21;22(1):157. doi: 10.1186/s12931-021-01750-8.
The long-term consequences of COVID-19 remain unclear. There is concern a proportion of patients will progress to develop pulmonary fibrosis. We aimed to assess the temporal change in CXR infiltrates in a cohort of patients following hospitalisation for COVID-19.
We conducted a single-centre prospective cohort study of patients admitted to University Hospital Southampton with confirmed SARS-CoV2 infection between 20th March and 3rd June 2020. Patients were approached for standard-of-care follow-up 12-weeks after hospitalisation. Inpatient and follow-up CXRs were scored by the assessing clinician for extent of pulmonary infiltrates; 0-4 per lung (Nil = 0, < 25% = 1, 25-50% = 2, 51-75% = 3, > 75% = 4).
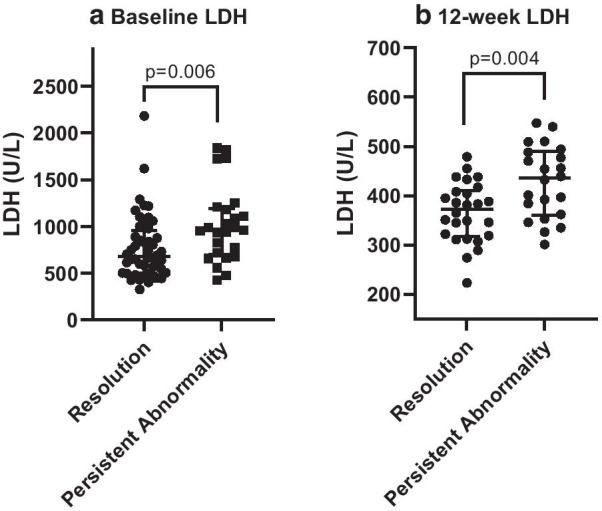
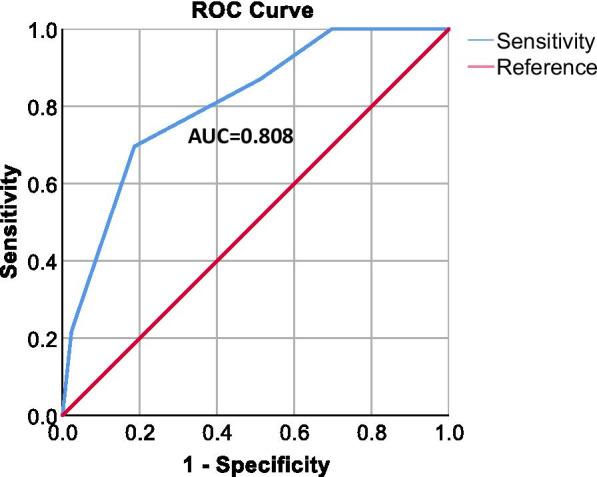
101 patients with paired CXRs were included. Demographics: 53% male with a median (IQR) age 53.0 (45-63) years and length of stay 9 (5-17.5) days. The median CXR follow-up interval was 82 (77-86) days with median baseline and follow-up CXR scores of 4.0 (3-5) and 0.0 (0-1) respectively. 32% of patients had persistent CXR abnormality at 12-weeks. In multivariate analysis length of stay (LOS), smoking-status and obesity were identified as independent risk factors for persistent CXR abnormality. Serum LDH was significantly higher at baseline and at follow-up in patients with CXR abnormalities compared to those with resolution. A 5-point composite risk score (1-point each; LOS ≥ 15 days, Level 2/3 admission, LDH > 750 U/L, obesity and smoking-status) strongly predicted risk of persistent radiograph abnormality (0.81).
Persistent CXR abnormality 12-weeks post COVID-19 was common in this cohort. LOS, obesity, increased serum LDH, and smoking-status were risk factors for radiograph abnormality. These findings require further prospective validation.
新型冠状病毒肺炎(COVID-19)的长期后果尚不清楚。人们担心一部分患者会进展为肺纤维化。我们旨在评估COVID-19住院患者队列中胸部X线(CXR)浸润的时间变化。
我们对2020年3月20日至6月3日期间入住南安普敦大学医院且确诊感染严重急性呼吸综合征冠状病毒2(SARS-CoV-2)的患者进行了一项单中心前瞻性队列研究。患者在住院12周后接受标准护理随访。评估医生对住院期间和随访时的胸部X线片进行评分,以确定肺部浸润程度;每侧肺0 - 4分(无浸润 = 0分,<25% = 1分,25% - 50% = 2分,51% - 75% = 3分,>75% = 4分)。
纳入了101例有配对胸部X线片的患者。人口统计学特征:53%为男性,中位(四分位间距)年龄53.0(45 - 63)岁,住院时间9(5 - 17.5)天。胸部X线片随访间隔的中位数为82(77 - 86)天,基线和随访时胸部X线片评分的中位数分别为4.0(3 - 5)分和0.0(0 - 1)分。32%的患者在12周时胸部X线片仍有异常。多因素分析显示,住院时间、吸烟状况和肥胖被确定为胸部X线片持续异常的独立危险因素。与胸部X线片异常已缓解的患者相比,胸部X线片异常患者在基线和随访时血清乳酸脱氢酶(LDH)显著更高。一个5分的综合风险评分(每项1分;住院时间≥15天、2/3级入院、LDH>750 U/L、肥胖和吸烟状况)能强烈预测胸部X线片持续异常的风险(0.81)。
在该队列中,COVID-19感染12周后胸部X线片持续异常很常见。住院时间、肥胖、血清LDH升高和吸烟状况是胸部X线片异常的危险因素。这些发现需要进一步的前瞻性验证。