Peretto Giovanni, Villatore Andrea, Rizzo Stefania, Esposito Antonio, De Luca Giacomo, Palmisano Anna, Vignale Davide, Cappelletti Alberto Maria, Tresoldi Moreno, Campochiaro Corrado, Sartorelli Silvia, Ripa Marco, De Gaspari Monica, Busnardo Elena, Ferro Paola, Calabrò Maria Grazia, Fominskiy Evgeny, Monaco Fabrizio, Cavalli Giulio, Gianolli Luigi, De Cobelli Francesco, Margonato Alberto, Dagna Lorenzo, Scandroglio Mara, Camici Paolo Guido, Mazzone Patrizio, Della Bella Paolo, Basso Cristina, Sala Simone
Department of Cardiac Electrophysiology and Arrhythmology, IRCCS San Raffaele Scientific Institute, 20132 Milan, Italy.
Myocarditis Disease Unit, IRCCS San Raffaele Scientific Institute, 20132 Milan, Italy.
J Clin Med. 2021 May 4;10(9):1974. doi: 10.3390/jcm10091974.
Myocarditis lacks systematic characterization in COVID-19 patients.
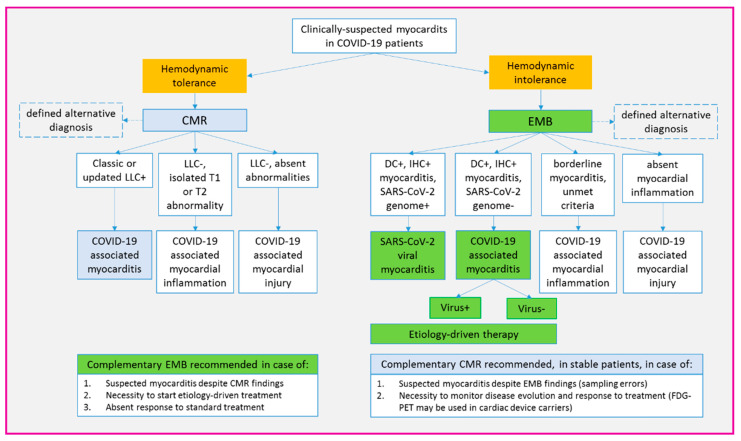
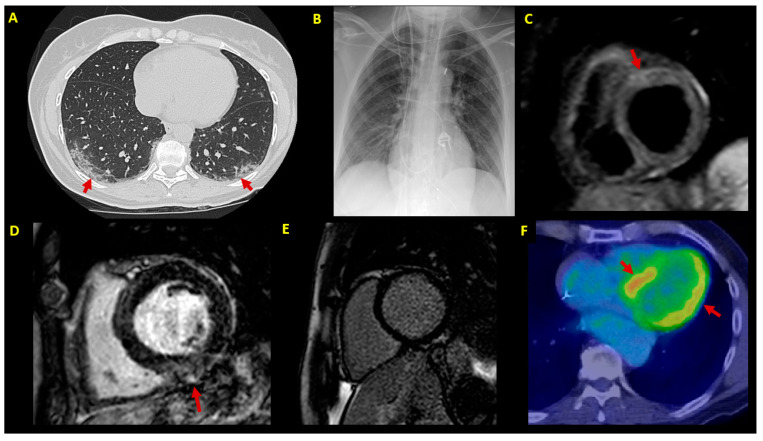
We enrolled consecutive patients with newly diagnosed myocarditis in the context of COVID-19 infection. Diagnostic and treatment strategies were driven by a dedicated multidisciplinary disease unit for myocarditis. Multimodal outcomes were assessed during prospective follow-up.
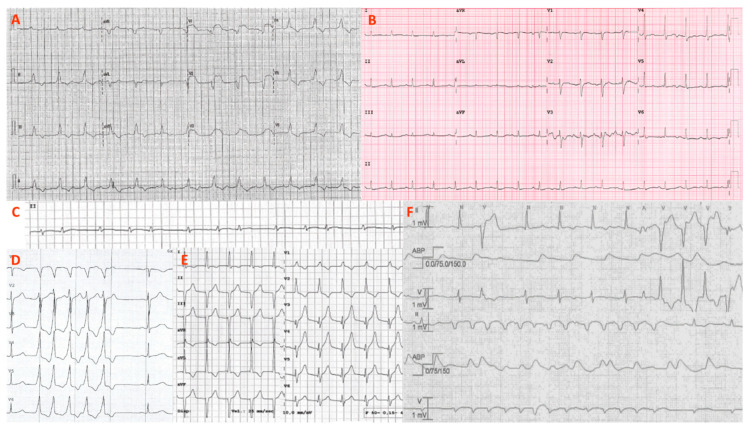
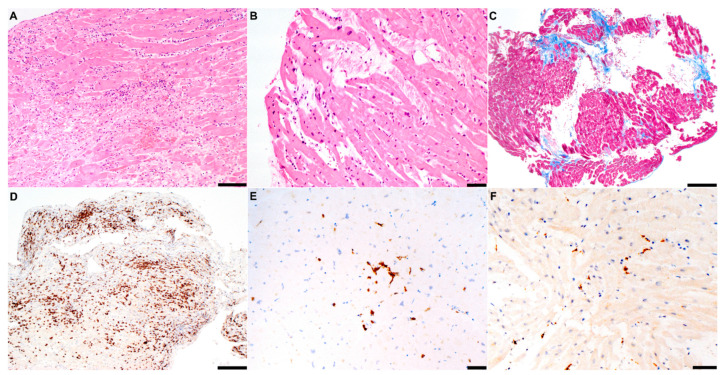
Seven consecutive patients (57% males, age 51 ± 9 y) with acute COVID-19 infection received a de novo diagnosis of myocarditis. Endomyocardial biopsy was of choice in hemodynamically unstable patients ( = 4, mean left ventricular ejection fraction (LVEF) 25 ± 9%), whereas cardiac magnetic resonance constituted the first exam in stable patients ( = 3, mean LVEF 48 ± 10%). Polymerase chain reaction (PCR) analysis revealed an intra-myocardial SARS-CoV-2 genome in one of the six cases undergoing biopsy: in the remaining patients, myocarditis was either due to other viruses ( = 2) or virus-negative ( = 3). Hemodynamic support was needed for four unstable patients (57%), whereas a cardiac device implant was chosen in two of four cases showing ventricular arrhythmias. Medical treatment included immunosuppression (43%) and biological therapy (29%). By the 6-month median follow-up, no patient died or experienced malignant arrhythmias. However, two cases (29%) were screened for heart transplantation.
Myocarditis associated with acute COVID-19 infection is a spectrum of clinical manifestations and underlying etiologies. A multidisciplinary approach is the cornerstone for tailored management.
新型冠状病毒肺炎(COVID-19)患者的心肌炎缺乏系统的特征描述。
我们纳入了在COVID-19感染背景下新诊断为心肌炎的连续患者。诊断和治疗策略由专门的心肌炎多学科疾病单元制定。在前瞻性随访期间评估多模式结局。
7例连续的急性COVID-19感染患者(男性占57%,年龄51±9岁)被重新诊断为心肌炎。对于血流动力学不稳定的患者(n = 4,平均左心室射血分数(LVEF)25±9%),心内膜心肌活检是首选,而心脏磁共振成像则是稳定患者(n = 3,平均LVEF 48±10%)的首选检查。聚合酶链反应(PCR)分析显示,在接受活检的6例患者中的1例心肌内存在严重急性呼吸综合征冠状病毒2(SARS-CoV-2)基因组;在其余患者中,心肌炎要么由其他病毒引起(n = 2),要么病毒检测为阴性(n = 3)。4例不稳定患者(57%)需要血流动力学支持,而在4例出现室性心律失常的患者中,有2例选择了植入心脏装置。药物治疗包括免疫抑制(43%)和生物治疗(29%)。到中位随访6个月时,无患者死亡或发生恶性心律失常。然而,有2例患者(29%)接受了心脏移植筛查。
与急性COVID-19感染相关的心肌炎具有一系列临床表现和潜在病因。多学科方法是进行个性化管理的基石。