Trials Centre, National Health and Medical Research Council Clinical Trials Centre, The University of Sydney, Sydney, NSW, 2006, Australia.
BMC Med Res Methodol. 2021 Jun 21;21(1):126. doi: 10.1186/s12874-021-01314-w.
Mortality is a key component of the natural history of COVID-19 infection. Surveillance data on COVID-19 deaths and case diagnoses are widely available in the public domain, but they are not used to model time to death because they typically do not link diagnosis and death at an individual level. This paper demonstrates that by comparing the unlinked patterns of new diagnoses and deaths over age and time, age-specific mortality and time to death may be estimated using a statistical method called deconvolution.
Age-specific data were analysed on 816 deaths among 6235 cases over age 50 years in Victoria, Australia, from the period January through December 2020. Deconvolution was applied assuming logistic dependence of case fatality risk (CFR) on age and a gamma time to death distribution. Non-parametric deconvolution analyses stratified into separate age groups were used to assess the model assumptions.
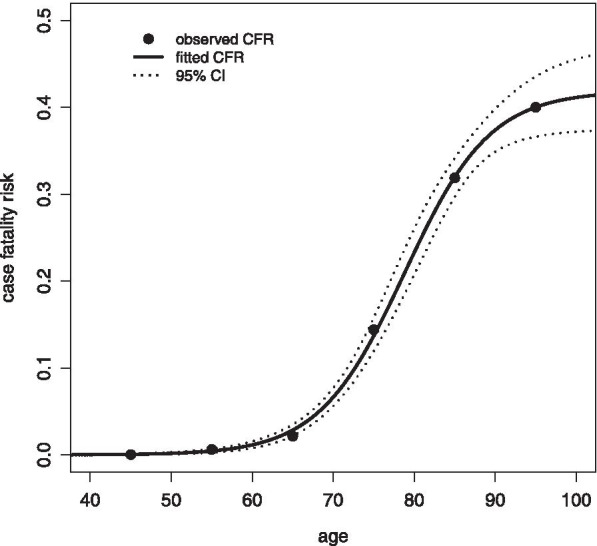
It was found that age-specific CFR rose from 2.9% at age 65 years (95% CI:2.2 - 3.5) to 40.0% at age 95 years (CI: 36.6 - 43.6). The estimated mean time between diagnosis and death was 18.1 days (CI: 16.9 - 19.3) and showed no evidence of varying by age (heterogeneity P = 0.97). The estimated 90% percentile of time to death was 33.3 days (CI: 30.4 - 36.3; heterogeneity P = 0.85). The final age-specific model provided a good fit to the observed age-stratified mortality patterns.
Deconvolution was demonstrated to be a powerful analysis method that could be applied to extensive data sources worldwide. Such analyses can inform transmission dynamics models and CFR assessment in emerging outbreaks. Based on these Australian data it is concluded that death from COVID-19 occurs within three weeks of diagnosis on average but takes five weeks in 10% of fatal cases. Fatality risk is negligible in the young but rises above 40% in the elderly, while time to death does not seem to vary by age.
死亡率是 COVID-19 感染自然史的一个关键组成部分。COVID-19 死亡和病例诊断的监测数据在公共领域广泛可用,但它们未被用于构建死亡时间模型,因为它们通常不能在个体层面上将诊断和死亡联系起来。本文证明,通过比较年龄和时间上的新诊断和死亡的非链接模式,可以使用一种称为反卷积的统计方法来估计特定年龄的死亡率和死亡时间。
对 2020 年 1 月至 12 月期间澳大利亚维多利亚州年龄在 50 岁以上的 6235 例病例中的 816 例死亡进行了特定年龄的数据分析。应用反卷积时,假设病例死亡率(CFR)的风险对数依赖性(logistic dependence)随年龄和伽马死亡时间分布。使用分层的非参数反卷积分析来评估模型假设。
发现特定年龄的 CFR 从 65 岁时的 2.9%(95%CI:2.2-3.5)上升到 95 岁时的 40.0%(CI:36.6-43.6)。诊断与死亡之间的估计平均时间为 18.1 天(CI:16.9-19.3),并且没有证据表明年龄存在差异(异质性 P=0.97)。估计的死亡时间 90%分位数为 33.3 天(CI:30.4-36.3;异质性 P=0.85)。最终的特定年龄模型与观察到的分层死亡率模式拟合良好。
证明反卷积是一种强大的分析方法,可应用于全球广泛的数据来源。此类分析可以为新兴暴发中的传播动力学模型和 CFR 评估提供信息。基于这些澳大利亚数据,可以得出结论,COVID-19 死亡平均在诊断后三周内发生,但在 10%的致死病例中需要五周时间。年轻人的病死率可以忽略不计,但在老年人中超过 40%,而死亡时间似乎不受年龄影响。