Department of Population Medicine, University of Guelph, Guelph, Ontario, Canada.
Department of Health Security, National Institute for Health and Welfare, Helsinki, Finland.
BMC Infect Dis. 2021 Jun 25;21(1):606. doi: 10.1186/s12879-021-06326-x.
Escherichia coli is the most common cause of bloodstream infections (BSIs) and mortality is an important aspect of burden of disease. Using a multinational population-based cohort of E. coli BSIs, our objectives were to evaluate 30-day case fatality risk and mortality rate, and determine factors associated with each.
During 2014-2018, we identified 30-day deaths from all incident E. coli BSIs from surveillance nationally in Finland, and regionally in Sweden (Skaraborg) and Canada (Calgary, Sherbrooke, western interior). We used a multivariable logistic regression model to estimate factors associated with 30-day case fatality risk. The explanatory variables considered for inclusion were year (2014-2018), region (five areas), age (< 70-years-old, ≥70-years-old), sex (female, male), third-generation cephalosporin (3GC) resistance (susceptible, resistant), and location of onset (community-onset, hospital-onset). The European Union 28-country 2018 population was used to directly age and sex standardize mortality rates. We used a multivariable Poisson model to estimate factors associated with mortality rate, and year, region, age and sex were considered for inclusion.
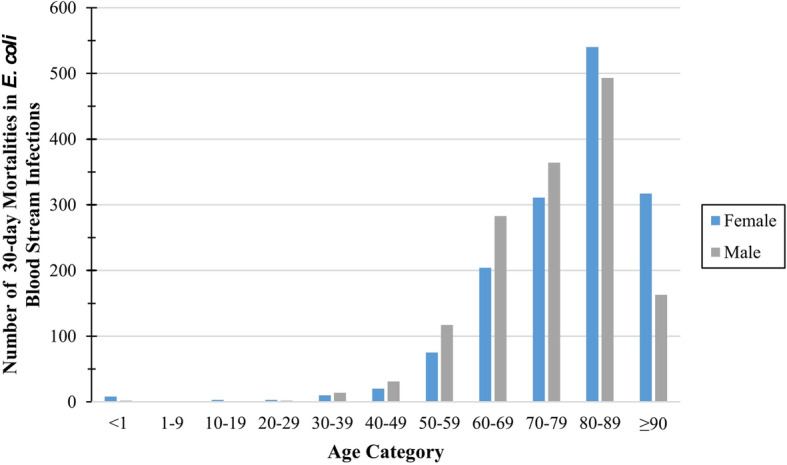
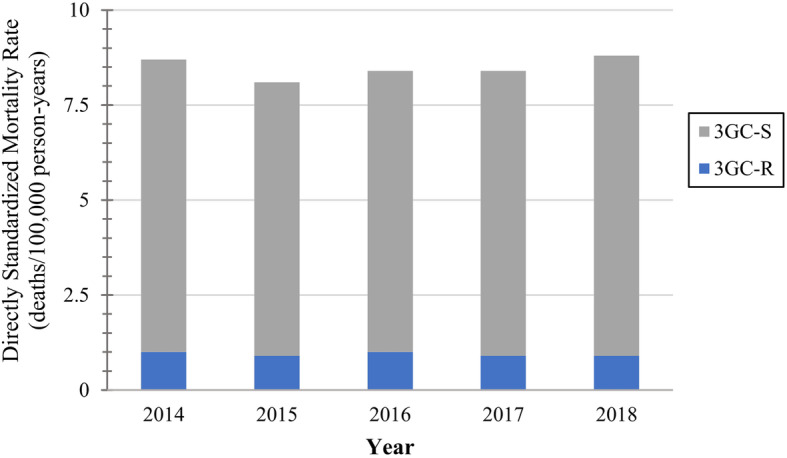
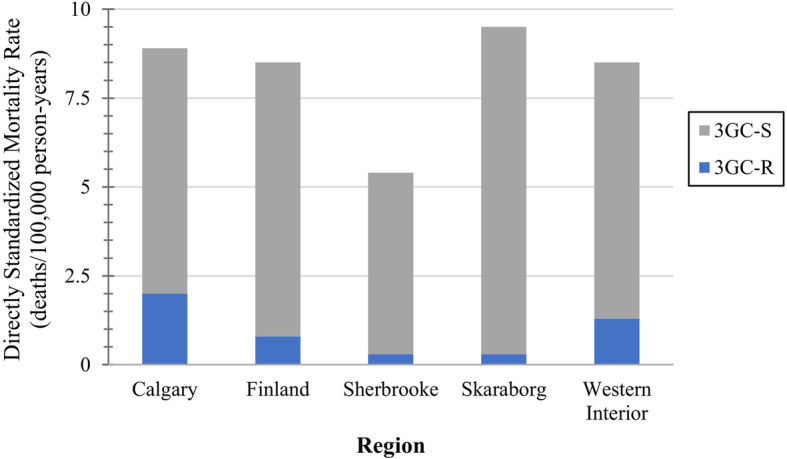
From 38.7 million person-years of surveillance, we identified 2961 30-day deaths in 30,923 incident E. coli BSIs. The overall 30-day case fatality risk was 9.6% (2961/30923). Calgary, Skaraborg, and western interior had significantly increased odds of 30-day mortality compared to Finland. Hospital-onset and 3GC-resistant E. coli BSIs had significantly increased odds of mortality compared to community-onset and 3GC-susceptible. The significant association between age and odds of mortality varied with sex, and contrasts were used to interpret this interaction relationship. The overall standardized 30-day mortality rate was 8.5 deaths/100,000 person-years. Sherbrooke had a significantly lower 30-day mortality rate compared to Finland. Patients that were either ≥70-years-old or male both experienced significantly higher mortality rates than those < 70-years-old or female.
In our study populations, region, age, and sex were significantly associated with both 30-day case fatality risk and mortality rate. Additionally, 3GC resistance and location of onset were significantly associated with 30-day case fatality risk. Escherichia coli BSIs caused a considerable burden of disease from 30-day mortality. When analyzing population-based mortality data, it is important to explore mortality through two lenses, mortality rate and case fatality risk.
大肠埃希菌是血流感染(BSI)最常见的原因,死亡率是疾病负担的一个重要方面。本研究通过对多国基于人群的大肠埃希菌血流感染队列进行分析,旨在评估 30 天病死率和死亡率,并确定与两者相关的因素。
2014 年至 2018 年期间,我们在芬兰全国范围内和瑞典(斯科讷省)和加拿大(卡尔加里、舍布鲁克、西部内陆)地区的区域监测中,确定了所有大肠埃希菌血流感染 30 天内的死亡病例。我们使用多变量逻辑回归模型来评估与 30 天病死率相关的因素。考虑纳入的解释变量包括年份(2014-2018 年)、地区(五个地区)、年龄(<70 岁,≥70 岁)、性别(女性、男性)、第三代头孢菌素(3GC)耐药性(敏感、耐药)和发病部位(社区发病、医院发病)。我们使用欧盟 28 国 2018 年的人口数据直接对死亡率进行年龄和性别标准化。我们使用多变量泊松模型来估计与死亡率相关的因素,纳入的因素包括年份、地区、年龄和性别。
在 3870 万个人监测年中,我们在 30923 例大肠埃希菌血流感染中确定了 2961 例 30 天内死亡病例。总体 30 天病死率为 9.6%(2961/30923)。与芬兰相比,卡尔加里、斯科讷省和西部内陆的 30 天死亡率明显更高。与社区发病和 3GC 敏感相比,医院发病和 3GC 耐药的大肠埃希菌血流感染的死亡率明显更高。年龄与死亡率之间的显著关联因性别而异,我们使用对比来解释这种交互关系。总体标准化 30 天死亡率为 8.5 例/10 万人口年。舍布鲁克与芬兰相比,30 天死亡率明显较低。≥70 岁或男性的患者死亡率明显高于<70 岁或女性患者。
在我们的研究人群中,地区、年龄和性别与 30 天病死率和死亡率均显著相关。此外,3GC 耐药和发病部位与 30 天病死率显著相关。大肠埃希菌血流感染导致 30 天死亡率造成了相当大的疾病负担。在分析基于人群的死亡率数据时,通过死亡率和病死率两个角度来探索死亡率非常重要。