Bonifay Timothee, Godaert Lidvine, Epelboin Yanouk, Rousset Dominique, Douine Maylis, Hilderal Hélène, Clavel Cyril, Abel Sylvie, Najioullah Fatiha, Fagour Laurence, do Socorro Mendonça Gomes Margarete, Lacerda Marcus, Cézaire Raymond, Elenga Narcisse, Dramé Moustapha, Hoen Bruno, Cabié André, Djossou Félix, Epelboin Loïc
Centre d'Investigation Clinique Antilles Guyane, INSERM 1424, Centre Hospitalier de Cayenne, Cayenne, French Guiana.
Short-stay Unit, Department of Geriatrics, General Hospital of Valenciennes, Valenciennes, France.
Curr Trop Med Rep. 2021;8(3):164-172. doi: 10.1007/s40475-021-00242-5. Epub 2021 Jun 19.
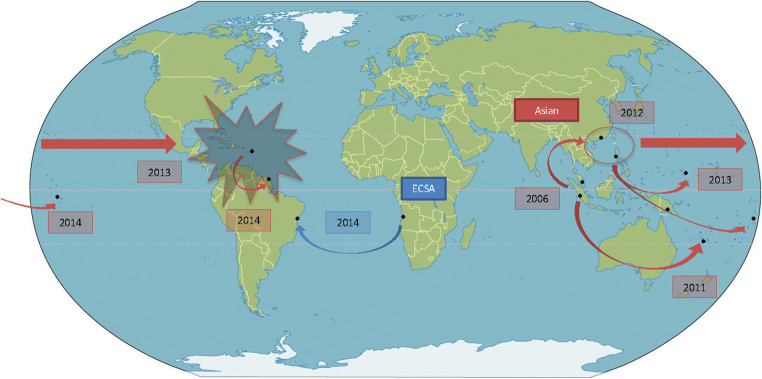
Although the chikungunya virus was discovered more than 60 years ago, it has only really been studied since the outbreak in La Reunion in 2005-2006. Ten years later, between 2014 and 2015, the chikungunya virus spread throughout the Americas, affecting millions of people. The objective of this review is to describe the contributions of research on chikungunya virus infection gained from epidemic in the West Indies and the Guiana Shield.
Prevalence data were similar to those found in the Indian Ocean or Asia during epidemics. Clinically, there is now a better understanding of the typical, atypical, and severe forms. Several studies have insisted on the presence of neurological forms of chikungunya infection, such as encephalitis or Guillain-Barré syndrome. Cases of septic shock due to chikungunya virus as well as thrombotic thrombocytopenic purpura were described for the first time. Given the magnitude of the epidemic and the large number of people affected, this has led to a better description and new classifications of chikungunya virus infections in specific populations such as pregnant women, the elderly, and children. Several studies also described the behavior of populations faced with an emerging disease.
Current epidemiological data from tropical regions highlights the risk of spreading emerging diseases at higher latitudes, especially concerning arboviruses, since the vector is already established in many parts of northern countries. A better understanding of the disease and its epidemic dynamics will foster better management, the crucial importance of which was demonstrated during the COVID-19 epidemic.
尽管基孔肯雅病毒在60多年前就已被发现,但直到2005 - 2006年留尼汪岛爆发疫情后才真正开始对其进行研究。十年后的2014年至2015年期间,基孔肯雅病毒在美洲蔓延,影响了数百万人。本综述的目的是描述从西印度群岛和圭亚那地盾的疫情中获得的关于基孔肯雅病毒感染研究的贡献。
流行率数据与印度洋或亚洲疫情期间的数据相似。在临床上,现在对典型、非典型和严重形式有了更好的理解。多项研究强调了基孔肯雅病毒感染存在神经学形式,如脑炎或吉兰 - 巴雷综合征。首次描述了由基孔肯雅病毒引起的感染性休克病例以及血栓性血小板减少性紫癜。鉴于疫情规模和受影响人数众多,这使得对孕妇、老年人和儿童等特定人群中的基孔肯雅病毒感染有了更好的描述和新的分类。多项研究还描述了人群面对新出现疾病时的行为。
热带地区目前的流行病学数据凸显了新兴疾病在高纬度地区传播的风险,尤其是对于虫媒病毒而言,因为其传播媒介已在许多北方国家的部分地区存在。对该疾病及其流行动态的更好理解将促进更好的管理,在2019冠状病毒病疫情期间已证明了其至关重要性。