Division of Epidemiology and Prevention, Institute of Human Virology, University of Maryland School of Medicine, 725 West Lombard Street, Room N345, MD, 21201, Baltimore, USA.
Institute of Human Virology, Center for International Health, Education, and Biosecurity (CIHEB), University of Maryland School of Medicine in Botswana, Gaborone, Botswana.
BMC Health Serv Res. 2021 Jul 20;21(1):711. doi: 10.1186/s12913-021-06731-7.
Scaling up continuous quality improvement (CQI) processes could be key in achieving the 95:95:95 cascade and global HIV targets. This paper describes the experiences and outcomes related to implementing CQI processes to help reach these targets, with particular focus on clinical and programmatic settings in 6 countries from the global south.
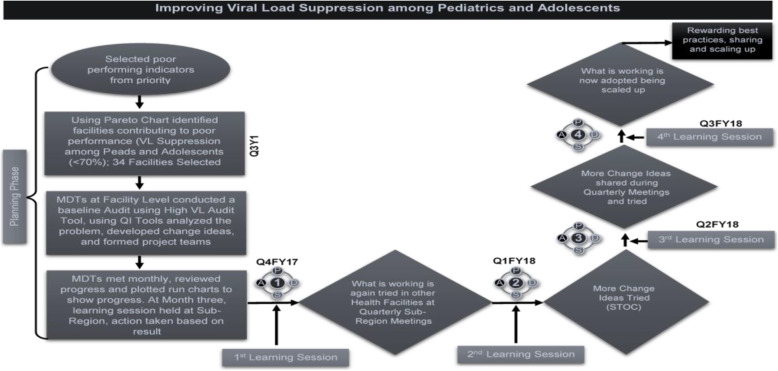
The HIV program at the University of Maryland, Baltimore (UMB) implemented an adapted CQI model in Kenya, Tanzania, Botswana, Zambia, Nigeria and Rwanda that included the following steps: (1) analysing the problem to identify goals and objectives for improvement; (2) developing individual changes or 'change packages', (3) developing a monitoring system to measure improvements; and (4) implementing and measuring changes through continuous 'plan-do-study-act' (PDSA) cycles. We describe country-level experiences related to implementing this adaptive design, a collaborative learning and scale-up/sustainability model that addresses the 95:95:95 global HIV targets via a CQI learning network, and mechanisms for fostering communication and the sharing of ideas and results; we describe trends both before and after model implementation.
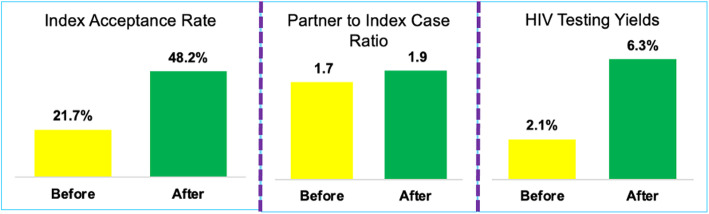
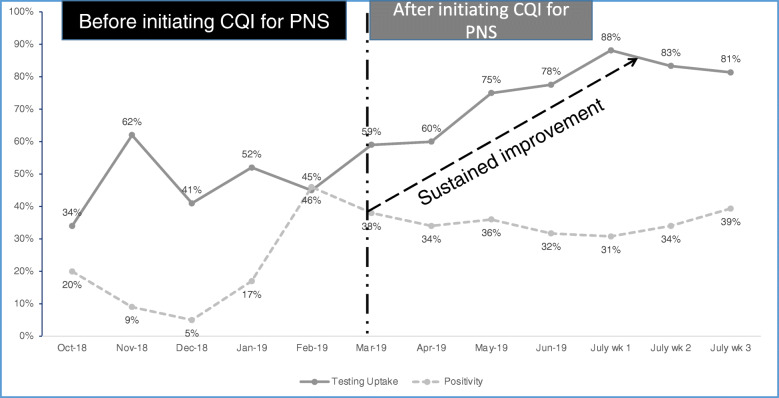
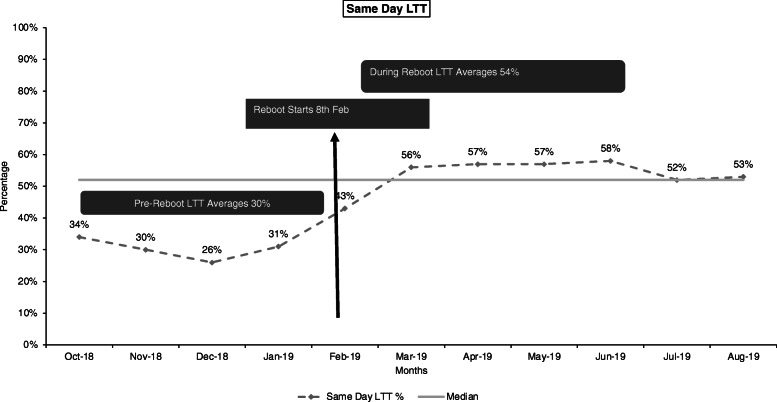
Our selected country-level experiences based on implementing our CQI approach resulted in an increased partner testing acceptance rate from 21.7 to 48.2 % in Rwanda, which resulted in an increase in the HIV testing yield from 2.1 to 6.3 %. In Botswana, the overall linkage to treatment improved from 63 to 94 %, while in Kenya, the viral load testing uptake among paediatric and adolescent patients improved from 65 to 96 %, and the viral load suppression improved from 53 to 88 %.
Adopting CQI processes is a useful approach for accelerating progress towards the attainment of the global 95:95:95 HIV targets. This paper also highlights the value of institutionalizing CQI processes and building the capacity of Ministry of Health (MoH) personnel in sub-Saharan Africa for the effective quality improvement of HIV programs and subsequent sustainability efforts.
扩大持续质量改进(CQI)流程可能是实现 95:95:95 级联和全球艾滋病毒目标的关键。本文描述了在 6 个来自全球南方的国家/地区的临床和规划环境中实施 CQI 流程以帮助实现这些目标的经验和结果,重点关注临床和规划环境。
马里兰大学巴尔的摩分校(UMB)的艾滋病毒项目在肯尼亚、坦桑尼亚、博茨瓦纳、赞比亚、尼日利亚和卢旺达实施了经改编的 CQI 模型,其中包括以下步骤:(1)分析问题以确定改进的目标和目标;(2)制定个人变革或“变革包”;(3)制定监测系统以衡量改进;(4)通过持续的“计划-执行-研究-行动”(PDSA)循环实施和衡量变革。我们描述了实施这种自适应设计的国家一级经验,这是一种协作学习和扩大规模/可持续性模型,通过 CQI 学习网络解决 95:95:95 全球艾滋病毒目标,并建立促进沟通以及分享想法和结果的机制;我们描述了模型实施前后的趋势。
我们根据实施 CQI 方法选择的国家一级经验导致卢旺达的合作伙伴检测接受率从 21.7%提高到 48.2%,这导致艾滋病毒检测率从 2.1%提高到 6.3%。在博茨瓦纳,总体治疗联系率从 63%提高到 94%,而在肯尼亚,儿科和青少年患者的病毒载量检测率从 65%提高到 96%,病毒载量抑制率从 53%提高到 88%。
采用 CQI 流程是加速实现全球 95:95:95 艾滋病毒目标的有用方法。本文还强调了将 CQI 流程制度化和建设撒哈拉以南非洲国家卫生部(MoH)人员能力的价值,以有效改进艾滋病毒规划的质量并随后进行可持续性努力。