Faculty of Epidemiology and Population Health, London School of Hygiene and Tropical Medicine, London, United Kingdom.
Division of Infection and Immunity, University College London, London, United Kingdom.
Clin Infect Dis. 2022 Aug 24;75(1):e1120-e1127. doi: 10.1093/cid/ciab754.
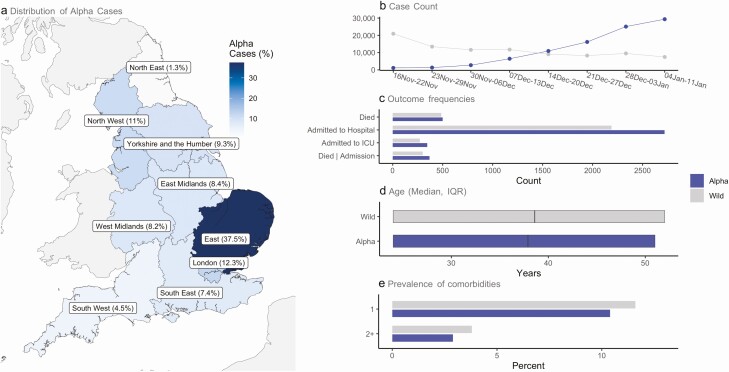
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) alpha variant (B.1.1.7) is associated with higher transmissibility than wild-type virus, becoming the dominant variant in England by January 2021. We aimed to describe the severity of the alpha variant in terms of the pathway of disease from testing positive to hospital admission and death.
With the approval of NHS England, we linked individual-level data from primary care with SARS-CoV-2 community testing, hospital admission, and Office for National Statistics all-cause death data. We used testing data with S-gene target failure as a proxy for distinguishing alpha and wild-type cases, and stratified Cox proportional hazards regression to compare the relative severity of alpha cases with wild-type diagnosed from 16 November 2020 to 11 January 2021.
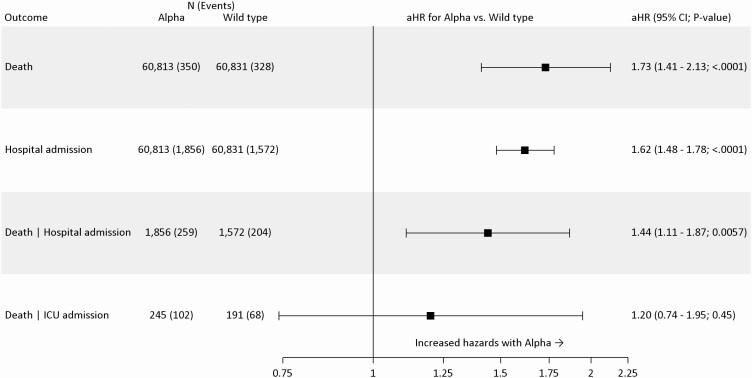
Using data from 185 234 people who tested positive for SARS-CoV-2 in the community (alpha = 93 153; wild-type = 92 081), in fully adjusted analysis accounting for individual-level demographics and comorbidities as well as regional variation in infection incidence, we found alpha associated with 73% higher hazards of all-cause death (adjusted hazard ratio [aHR]: 1.73; 95% confidence interval [CI]: 1.41-2.13; P < .0001) and 62% higher hazards of hospital admission (1.62; 1.48-1.78; P < .0001) compared with wild-type virus. Among patients already admitted to the intensive care unit, the association between alpha and increased all-cause mortality was smaller and the CI included the null (aHR: 1.20; 95% CI: .74-1.95; P = .45).
The SARS-CoV-2 alpha variant is associated with an increased risk of both hospitalization and mortality than wild-type virus.
严重急性呼吸综合征冠状病毒 2 (SARS-CoV-2)的阿尔法变体(B.1.1.7)的传染性高于野生型病毒,到 2021 年 1 月成为英国的主要变体。我们旨在描述从检测呈阳性到住院和死亡的疾病途径中阿尔法变体的严重程度。
在获得英国国民保健署批准的情况下,我们将初级保健的个体数据与 SARS-CoV-2 社区检测、住院和国家统计局全因死亡数据进行了关联。我们使用 S 基因靶标失败作为区分阿尔法和野生型病例的代理,并使用分层 Cox 比例风险回归来比较 2020 年 11 月 16 日至 2021 年 1 月 11 日期间诊断出的阿尔法病例与野生型病例的相对严重程度。
使用社区中检测出的 185234 人感染 SARS-CoV-2 的数据(阿尔法病例=93153 例;野生型病例=92081 例),在完全调整后的分析中,我们考虑了个体水平的人口统计学和合并症以及感染发生率的区域差异,发现阿尔法病例与全因死亡的风险增加 73%相关(调整后的危险比[aHR]:1.73;95%置信区间[CI]:1.41-2.13;P<0.0001),与住院的风险增加 62%相关(1.62;1.48-1.78;P<0.0001),与野生型病毒相比。在已经被收入重症监护病房的患者中,阿尔法与全因死亡率增加之间的关联较小,且 CI 包含零值(aHR:1.20;95%CI:0.74-1.95;P=0.45)。
与野生型病毒相比,SARS-CoV-2 的阿尔法变体与住院和死亡率增加的风险均相关。