Chen Simiao, Sun Hui, Heng Mei, Tong Xunliang, Geldsetzer Pascal, Wang Zhuoran, Wu Peixin, Yang Juntao, Hu Yu, Wang Chen, Bärnighausen Till
Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing 100730, China.
Heidelberg Institute of Global Health (HIGH), Faculty of Medicine and University Hospital, Heidelberg University, Heidelberg 69120, Germany.
Engineering (Beijing). 2022 Jun;13:99-106. doi: 10.1016/j.eng.2021.07.021. Epub 2021 Oct 23.
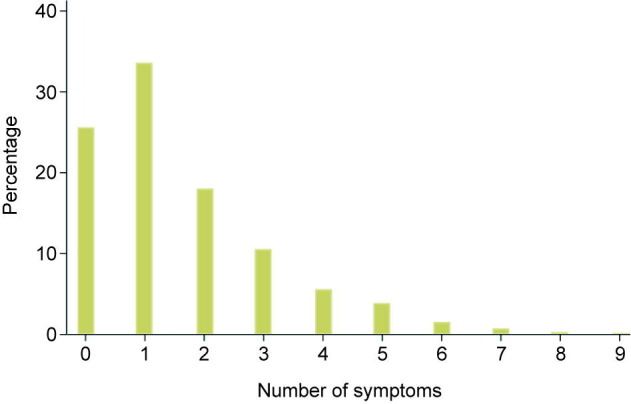
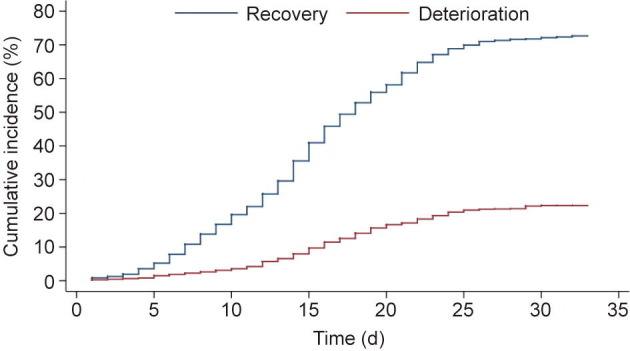
Most studies of coronavirus disease 2019 (COVID-19) progression have focused on the transfer of patients within secondary or tertiary care hospitals from regular wards to intensive care units. Little is known about the risk factors predicting the progression to severe COVID-19 among patients in community isolation, who are either asymptomatic or suffer from only mild to moderate symptoms. Using a multivariable competing risk survival analysis, we identify several important predictors of progression to severe COVID-19-rather than to recovery-among patients in the largest community isolation center in Wuhan, China from 6 February 2020 (when the center opened) to 9 March 2020 (when it closed). All patients in community isolation in Wuhan were either asymptomatic or suffered from mild to moderate COVID-19 symptoms. We performed competing risk survival analysis on time-to-event data from a cohort study of all COVID-19 patients ( = 1753) in the isolation center. The potential predictors we investigated were the routine patient data collected upon admission to the isolation center: age, sex, respiratory symptoms, gastrointestinal symptoms, general symptoms, and computed tomography (CT) scan signs. The main outcomes were time to severe COVID-19 or recovery. The factors predicting progression to severe COVID-19 were: male sex (hazard ratio (HR) = 1.29, 95% confidence interval (CI) 1.04-1.58, = 0.018), young and old age, dyspnea (HR = 1.58, 95% CI 1.24-2.01, < 0.001), and CT signs of ground-glass opacity (HR = 1.39, 95% CI 1.04-1.86, = 0.024) and infiltrating shadows (HR = 1.84, 95% CI 1.22-2.78, = 0.004). The risk of progression was found to be lower among patients with nausea or vomiting (HR = 0.53, 95% CI 0.30-0.96, = 0.036) and headaches (HR = 0.54, 95% CI 0.29-0.99, = 0.046). Our results suggest that several factors that can be easily measured even in resource-poor settings (dyspnea, sex, and age) can be used to identify mild COVID-19 patients who are at increased risk of disease progression. Looking for CT signs of ground-glass opacity and infiltrating shadows may be an affordable option to support triage decisions in resource-rich settings. Common and unspecific symptoms (headaches, nausea, and vomiting) are likely to have led to the identification and subsequent community isolation of COVID-19 patients who were relatively unlikely to deteriorate. Future public health and clinical guidelines should build on this evidence to improve the screening, triage, and monitoring of COVID-19 patients who are asymtomatic or suffer from mild to moderate symptoms.
大多数关于2019冠状病毒病(COVID-19)病情进展的研究都集中在二级或三级护理医院内患者从普通病房转至重症监护病房的情况。对于社区隔离的患者(这些患者要么无症状,要么仅患有轻度至中度症状)中预测COVID-19病情进展为重症的风险因素,人们了解甚少。我们采用多变量竞争风险生存分析,在中国武汉最大的社区隔离中心,对2020年2月6日(该中心开放之日)至2020年3月9日(该中心关闭之日)期间的患者,确定了几个导致COVID-19病情进展为重症而非康复的重要预测因素。武汉所有社区隔离患者均无症状或患有轻度至中度COVID-19症状。我们对隔离中心所有COVID-19患者(n = 1753)队列研究的事件发生时间数据进行了竞争风险生存分析。我们调查的潜在预测因素为患者入住隔离中心时收集的常规数据:年龄、性别、呼吸道症状、胃肠道症状、一般症状以及计算机断层扫描(CT)征象。主要结局为进展为重症COVID-19或康复的时间。预测进展为重症COVID-19的因素包括:男性(风险比(HR)= 1.29,95%置信区间(CI)1. .04 - 1.58,P = 0.018)、年龄偏大或偏小、呼吸困难(HR = 1.58,95% CI 1.24 - 2.01,P < 0.001)以及CT表现为磨玻璃影(HR = 1.39,95% CI 1.04 - 1.86,P = 0.024)和浸润影(HR = 1.84,95% CI 1.22 - 2.78,P = 0.004)。恶心或呕吐患者(HR = 0.53,95% CI 0.30 - 0.96,P = 0.036)和头痛患者(HR = 0.54,95% CI 0.29 - 0.99,P = 0.046)病情进展风险较低。我们的结果表明,即使在资源匮乏的环境中也易于测量的几个因素(呼吸困难、性别和年龄)可用于识别疾病进展风险增加的轻症COVID-19患者。寻找磨玻璃影和浸润影的CT征象可能是在资源丰富环境中支持分诊决策的一种经济实惠的选择。常见且非特异性症状(头痛、恶心和呕吐)可能促使识别出相对不太可能病情恶化的COVID-19患者并随后对其进行社区隔离。未来的公共卫生和临床指南应基于这一证据,以改善对无症状或患有轻度至中度症状的COVID-19患者的筛查、分诊和监测。