Heart and Vascular Center, Semmelweis University, Budapest, Hungary.
Department of Sports Medicine, Semmelweis University, Budapest, Hungary.
Br J Sports Med. 2022 May;56(10):553-560. doi: 10.1136/bjsports-2021-104576. Epub 2021 Nov 30.
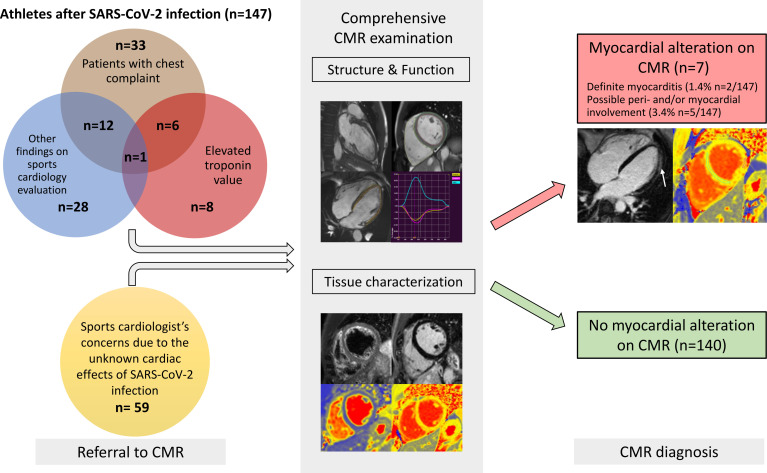
To investigate the cardiovascular consequences of SARS-CoV-2 infection in highly trained, otherwise healthy athletes using cardiac magnetic resonance (CMR) imaging and to compare our results with sex-matched and age-matched athletes and less active controls.
SARS-CoV-2 infection was diagnosed by PCR on swab tests or serum immunoglobulin G antibody tests prior to a comprehensive CMR examination. The CMR protocol contained sequences to assess structural, functional and tissue-specific data.
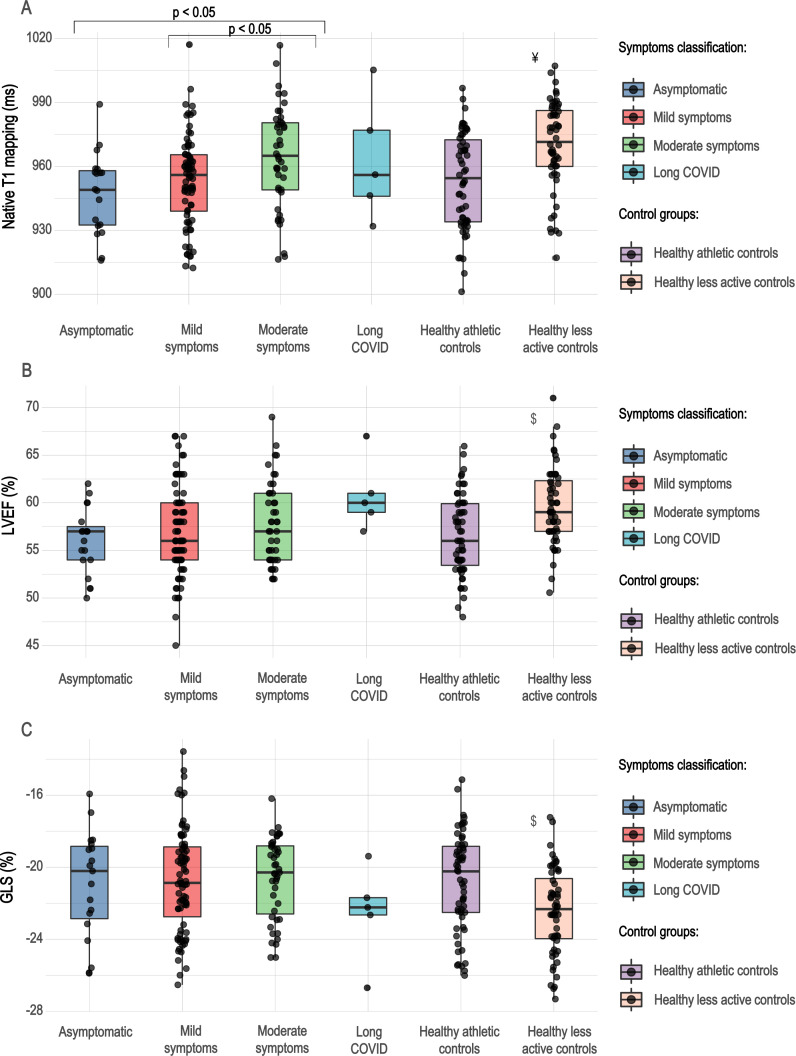
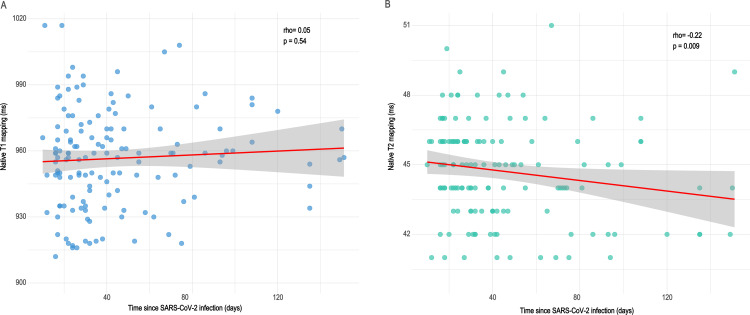
One hundred forty-seven athletes (94 male, median 23, IQR 20-28 years) after SARS-CoV-2 infection were included. Overall, 4.7% (n=7) of the athletes had alterations in their CMR as follows: late gadolinium enhancement (LGE) showing a non-ischaemic pattern with or without T2 elevation (n=3), slightly elevated native T1 values with or without elevated T2 values without pathological LGE (n=3) and pericardial involvement (n=1). Only two (1.4%) athletes presented with definite signs of myocarditis. We found pronounced sport adaptation in both athletes after SARS-CoV-2 infection and athlete controls. There was no difference between CMR parameters, including native T1 and T2 mapping, between athletes after SARS-CoV-2 infection and the matched athletic groups. Comparing athletes with different symptom severities showed that athletes with moderate symptoms had slightly greater T1 values than athletes with asymptomatic and mildly symptomatic infections (p<0.05). However, T1 mapping values remained below the cut-off point for most patients.
Among 147 highly trained athletes after SARS-CoV-2 infection, cardiac involvement on CMR showed a modest frequency (4.7%), with definite signs of myocarditis present in only 1.4%. Comparing athletes after SARS-CoV-2 infection and healthy sex-matched and age-matched athletes showed no difference between CMR parameters, including native T1 and T2 values.
使用心脏磁共振(CMR)成像研究 SARS-CoV-2 感染对高度训练、健康的运动员的心血管后果,并将我们的结果与性别匹配和年龄匹配的运动员和活动较少的对照组进行比较。
在进行全面的 CMR 检查之前,通过拭子检测或血清免疫球蛋白 G 抗体检测诊断 SARS-CoV-2 感染。CMR 方案包含用于评估结构、功能和组织特异性数据的序列。
共纳入 147 名 SARS-CoV-2 感染后的运动员(94 名男性,中位数 23 岁,IQR 20-28 岁)。总体而言,4.7%(n=7)的运动员的 CMR 出现以下改变:晚期钆增强(LGE)呈非缺血性模式,伴有或不伴有 T2 升高(n=3)、轻微升高的固有 T1 值伴有或不伴有升高的 T2 值而无病理性 LGE(n=3)和心包受累(n=1)。仅有 2 名(1.4%)运动员出现明确的心肌炎征象。我们发现 SARS-CoV-2 感染后和运动员对照组的运动员都有明显的运动适应。SARS-CoV-2 感染后运动员和匹配的运动员组之间的 CMR 参数(包括固有 T1 和 T2 图谱)没有差异。比较不同症状严重程度的运动员发现,症状中度的运动员的 T1 值略高于无症状和轻度症状感染的运动员(p<0.05)。然而,T1 映射值仍低于大多数患者的截止值。
在 147 名 SARS-CoV-2 感染后的高度训练的运动员中,CMR 上的心脏受累频率适中(4.7%),仅有 1.4%出现明确的心肌炎征象。比较 SARS-CoV-2 感染后的运动员和健康的性别匹配和年龄匹配的运动员,CMR 参数(包括固有 T1 和 T2 值)没有差异。