Center for Quality Control and Improvement of Physical Examination, Beijing Physical Examination Center, No. 1, Yard 81, Fucheng Road, Beijing, Haidian District, China.
Research Center of Digital Health China, Health and Medical Research Institute, Jinan, China.
BMC Endocr Disord. 2022 Feb 28;22(1):50. doi: 10.1186/s12902-022-00954-3.
High Blood Urea Nitrogen (BUN) and high Serum Creatinine (SCr) levels are risk factors for Coronary Artery Disease (CAD). However, the relationship between the Blood Urea Nitrogen to Creatinine (BUN/SCr) ratio (UCR) and the risk of CAD in patients living with new-onset diabetes is unclear. This study aimed to examine the relationship between blood UCR and the risk of CAD in patients living with new-onset type 2 diabetes mellitus (T2DM).
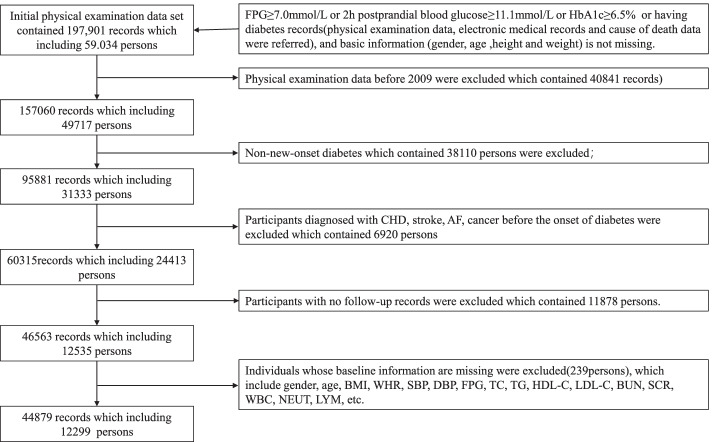
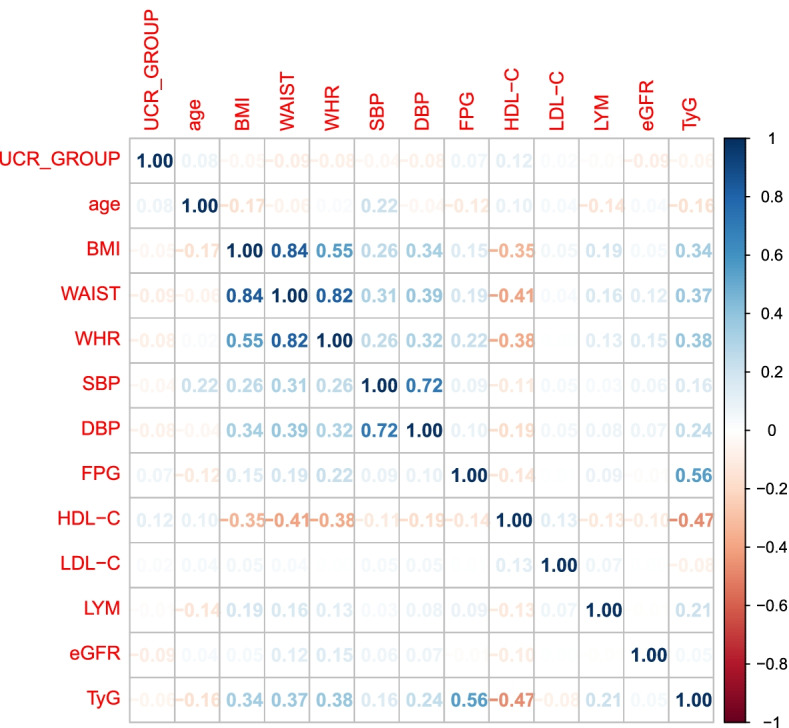
We analyzed the data from the cohort of 12,299 patients living with type 2 diabetes mellitus. Primary endpoints were the events of CAD. The ANOVA test (continuous indicators) and χ test (categorical indicators) were used to assess the differences of baseline characteristics across the groups of UCR. In order to understand the correlation between variables, we performed correlation analysis on variables that have significant differences between CAD group and non-CAD group. Multivariate-adjusted Cox proportional hazard regression models were applied to estimate the association of the blood UCR with the risk of CAD in patients living with T2DM. The Kaplan-Meier survival function plotting and the log-rank test were used to evaluate the event-free survival according to the groups of UCR. The restricted cubic spline model was used to show the adjusted association between blood UCR and risk of CAD in patients living with T2DM.
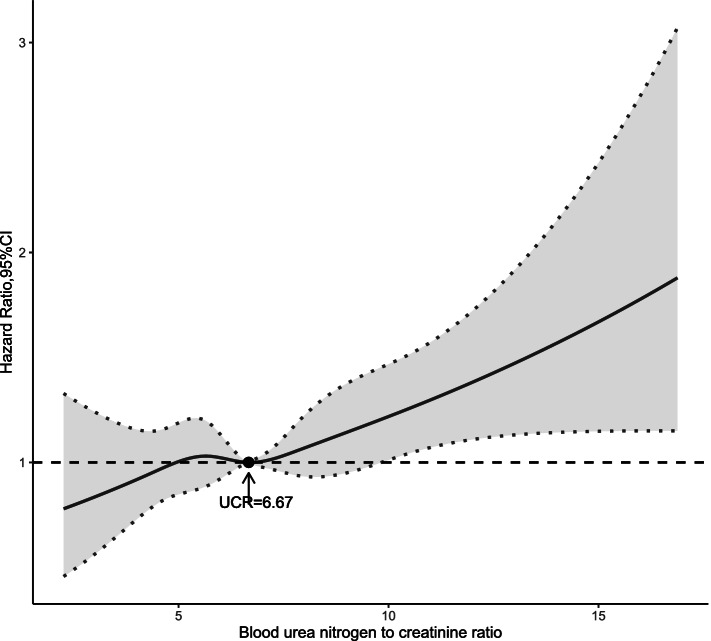
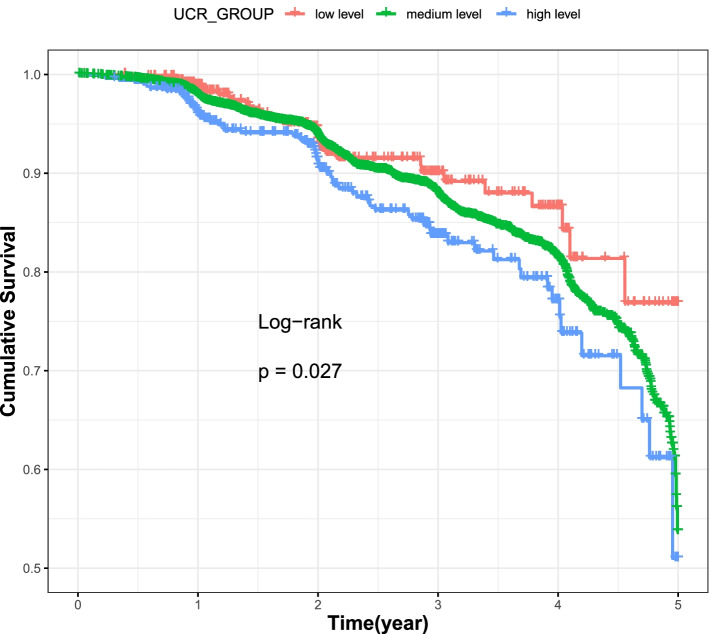
During a median follow-up of 2.66 years, 1173 CAD were recorded with an event rate of 28.49 events per 1000 person-years. In multivariate-adjusted Cox regression models, elevated blood urea nitrogen to creatinine ratio (UCR) was associated with higher risk of CAD in patients living with T2DM [hazard ratio (HR), 1.782; 95% confidence interval (CI), 1.237-2.567]. The Kaplan-Meier survival curves indicated that the high group of UCR tended to have a lower event-free survival than the low group and medium group. There was a nonlinear trend toward increasing risk of CAD across the groups of UCR. And cubic spline function graph suggested that the influence of UCR level on HR for CAD increased significantly at UCR levels above 6.67.
An elevated UCR was significantly associated with an increased risk for CAD in patients living with T2DM.
高血尿素氮(BUN)和高血清肌酐(SCr)水平是冠心病(CAD)的危险因素。然而,新诊断为糖尿病患者的血尿素氮与肌酐比值(UCR)与 CAD 风险之间的关系尚不清楚。本研究旨在探讨新诊断为 2 型糖尿病(T2DM)患者血 UCR 与 CAD 风险之间的关系。
我们分析了 12299 例 2 型糖尿病患者的队列数据。主要终点为 CAD 事件。采用方差分析(连续指标)和卡方检验(分类指标)比较 UCR 各组间基线特征的差异。为了了解变量之间的相关性,我们对 CAD 组和非 CAD 组之间有显著差异的变量进行了相关性分析。采用多变量调整的 Cox 比例风险回归模型来估计血 UCR 与 T2DM 患者 CAD 风险的相关性。采用 Kaplan-Meier 生存函数绘图和对数秩检验评估 UCR 组之间的无事件生存率。采用限制性立方样条模型显示血 UCR 与 T2DM 患者 CAD 风险之间的调整关联。
中位随访 2.66 年后,共记录 1173 例 CAD,事件发生率为每 1000 人年 28.49 例。在多变量调整的 Cox 回归模型中,升高的血尿素氮与肌酐比值(UCR)与 T2DM 患者 CAD 风险增加相关[风险比(HR),1.782;95%置信区间(CI),1.237-2.567]。Kaplan-Meier 生存曲线表明,UCR 较高组的无事件生存率低于 UCR 较低组和中等组。随着 UCR 组的增加,CAD 的风险呈非线性增加趋势。立方样条函数图表明,UCR 水平高于 6.67 时,UCR 水平对 CAD 的 HR 影响显著增加。
升高的 UCR 与 T2DM 患者 CAD 风险增加显著相关。