Division of Nephrology, Department of Medicine, Columbia University Irving Medical Center, New York, New York.
Vagelos College of Physicians and Surgeons, Columbia University, New York, New York.
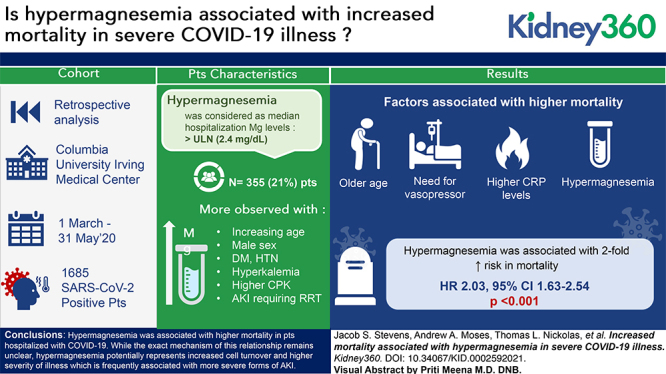
Kidney360. 2021 May 17;2(7):1087-1094. doi: 10.34067/KID.0002592021. eCollection 2021 Jul 29.
Although electrolyte abnormalities are common among patients with COVID-19, very little has been reported on magnesium homeostasis in these patients. Here we report the incidence of hypermagnesemia, and its association with outcomes among patients admitted with COVID-19.
We retrospectively identified all patients with a positive test result for SARS-CoV-2 who were admitted to a large quaternary care center in New York City in spring 2020. Details of the patients' demographics and hospital course were obtained retrospectively from medical records. Patients were defined as having hypermagnesemia if their median magnesium over the course of their hospitalization was >2.4 mg/dl.
A total of 1685 patients hospitalized with COVID-19 had their magnesium levels checked during their hospitalization, and were included in the final study cohort, among whom 355 (21%) had hypermagnesemia. Patients who were hypermagnesemic had a higher incidence of shock requiring pressors (35% vs 27%, <0.01), respiratory failure requiring mechanical ventilation (28% vs 21%, =0.01), AKI (65% vs 50%, <0.001), and AKI severe enough to require renal replacement therapy (18% vs 5%, <0.001). In an adjusted multivariable model, hypermagnesemia was observed more commonly with increasing age, male sex, AKI requiring RRT, hyperkalemia, and higher CPK. Survival probability at 30 days was 34% for the patients with hypermagnesemia, compared with 65% for patients without hypermagnesemia. An adjusted multivariable time to event analysis identified an increased risk of mortality with older age, need for vasopressors, higher C-reactive protein levels, and hypermagnesemia (HR, 2.03; 95% CI, 1.63 to 2.54, <0.001).
In conclusion, we identified an association between hypermagnesemia among patients hospitalized with COVID-19 and increased mortality. Although the exact mechanism of this relationship remains unclear, hypermagnesemia potentially represents increased cell turnover and higher severity of illness, which is frequently associated with more severe forms of AKI.
尽管 COVID-19 患者中电解质异常很常见,但关于这些患者的镁稳态的报道却很少。在这里,我们报告高镁血症的发生率及其与 COVID-19 住院患者结局的关系。
我们回顾性地确定了 2020 年春季在纽约市一家大型四级保健中心住院的 SARS-CoV-2 检测结果为阳性的所有患者。从病历中回顾性地获得了患者的人口统计学和住院过程的详细信息。如果患者住院期间的中位数镁水平>2.4mg/dl,则将其定义为高镁血症。
共有 1685 名患有 COVID-19 的患者在住院期间检查了其镁水平,并纳入了最终的研究队列,其中 355 名(21%)患有高镁血症。高镁血症患者休克需要升压药的发生率更高(35%比 27%,<0.01)、需要机械通气的呼吸衰竭发生率更高(28%比 21%,=0.01)、急性肾损伤发生率更高(65%比 50%,<0.001)、需要肾脏替代治疗的急性肾损伤发生率更高(18%比 5%,<0.001)。在调整后的多变量模型中,随着年龄的增加、男性、需要肾脏替代治疗的急性肾损伤、高钾血症和更高的肌酸磷酸激酶(CPK),观察到高镁血症的频率更高。高镁血症患者的 30 天生存率为 34%,而无高镁血症患者的生存率为 65%。调整后的时间事件分析确定,随着年龄的增加、需要升压药、C 反应蛋白水平升高和高镁血症,死亡率的风险增加(风险比[HR],2.03;95%置信区间[CI],1.63 至 2.54,<0.001)。
总之,我们发现 COVID-19 住院患者高镁血症与死亡率增加之间存在关联。尽管这种关系的确切机制尚不清楚,但高镁血症可能代表细胞更新增加和疾病严重程度增加,这通常与更严重形式的急性肾损伤有关。