Fayed Mohamed, Patel Nimesh, Angappan Santhalakshmi, Nowak Katherine, Vasconcelos Torres Felipe, Penning Donald H, Chhina Anoop K
Anesthesiology, Pain Management and Perioperative Medicine, Henry Ford Health System, Detroit, USA.
Anesthesia, Henry Ford Health System, Detroit, USA.
Cureus. 2022 Jul 16;14(7):e26911. doi: 10.7759/cureus.26911. eCollection 2022 Jul.
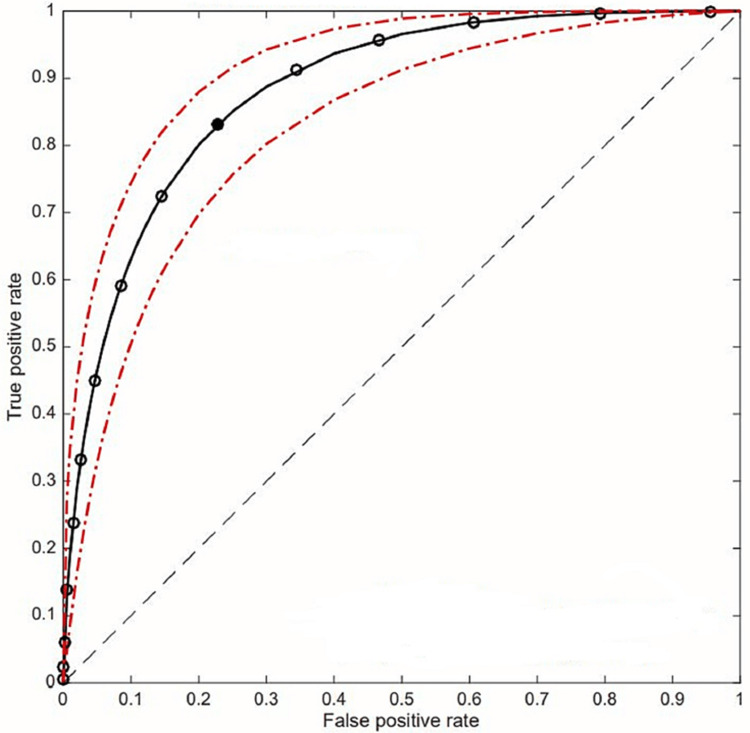
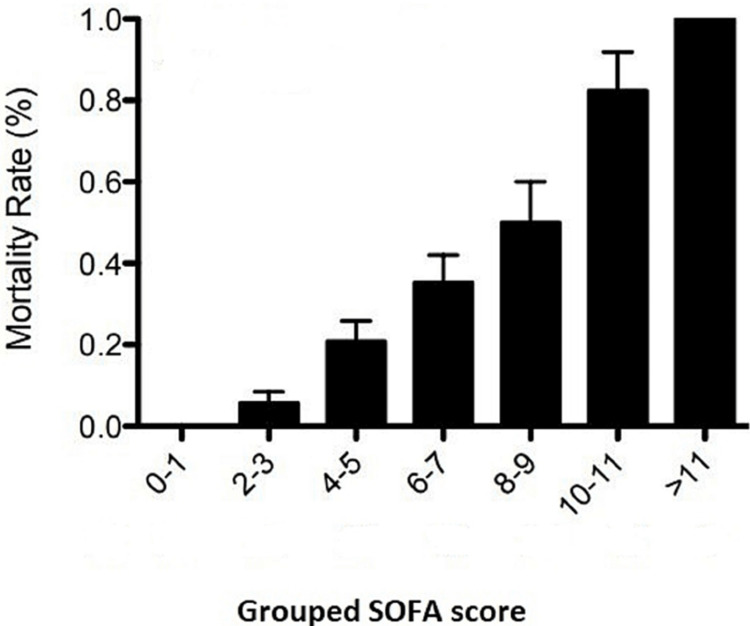
Background This study looks at the validity of the sequential organ failure assessment score (SOFA) in detecting mortality in patients with Coronavirus disease of 2019 (COVID-19) pneumonia. Also, it is looking to determine the optimal SOFA score that will discriminate between mortality and survival. Methods It is a retrospective chart review of the patients admitted to Henry Ford Hospital from March 2020 to December 2020 with COVID-19 pneumonia who developed severe respiratory distress. We collected the following information; patient demographics (age, sex, body mass index), co-morbidities (history of diabetes mellitus, chronic kidney disease, chronic obstructive pulmonary disease, coronary artery disease, or cancer), SOFA scores (the ratio of arterial oxygen tension (PaO) to the fraction of inspired oxygen, Glasgow Coma Scale (GCS) score, mean arterial pressure, serum creatinine level, bilirubin level, and platelet count) as well as inpatient mortality. Results There were 320 patients; out of these, 111 were intubated. The receiver operating characteristic (ROC) curve for SOFA at the moment of inclusion in the study had an area under the curve of 0.883. The optimal point for discrimination between mortality and survival is SOFA of 5. A SOFA score of less than two is associated with 100% survival, while a score of more than 11 is associated with 100% mortality. Conclusions SOFA score in COVID-19 patients with severe respiratory distress strongly correlates with the initial SOFA score. It is a valuable tool for predicting mortality in COVID-19 patients.
背景 本研究旨在探讨序贯器官衰竭评估评分(SOFA)在检测2019冠状病毒病(COVID-19)肺炎患者死亡率方面的有效性。此外,还试图确定能够区分死亡和存活的最佳SOFA评分。方法 这是一项对2020年3月至2020年12月因COVID-19肺炎并发严重呼吸窘迫而入住亨利福特医院的患者进行的回顾性病历审查。我们收集了以下信息:患者人口统计学资料(年龄、性别、体重指数)、合并症(糖尿病史、慢性肾脏病、慢性阻塞性肺疾病、冠状动脉疾病或癌症史)、SOFA评分(动脉血氧分压(PaO)与吸入氧分数之比、格拉斯哥昏迷量表(GCS)评分、平均动脉压、血清肌酐水平、胆红素水平和血小板计数)以及住院死亡率。结果 共有320例患者;其中111例接受了插管治疗。研究纳入时SOFA的受试者工作特征(ROC)曲线下面积为0.883。区分死亡和存活的最佳点是SOFA评分为5。SOFA评分低于2与100%的存活率相关,而评分高于11与100%的死亡率相关。结论 COVID-19并发严重呼吸窘迫患者的SOFA评分与初始SOFA评分密切相关。它是预测COVID-19患者死亡率的一个有价值的工具。