Department of Statistics, Florida State University, Tallahassee, FL, USA.
Cancer Epidemiology Division, Population Sciences in the Pacific Program, University of Hawaii Cancer Center, University of Hawaii at Manoa, Honolulu, HI, USA.
BMC Med. 2022 Nov 7;20(1):385. doi: 10.1186/s12916-022-02583-y.
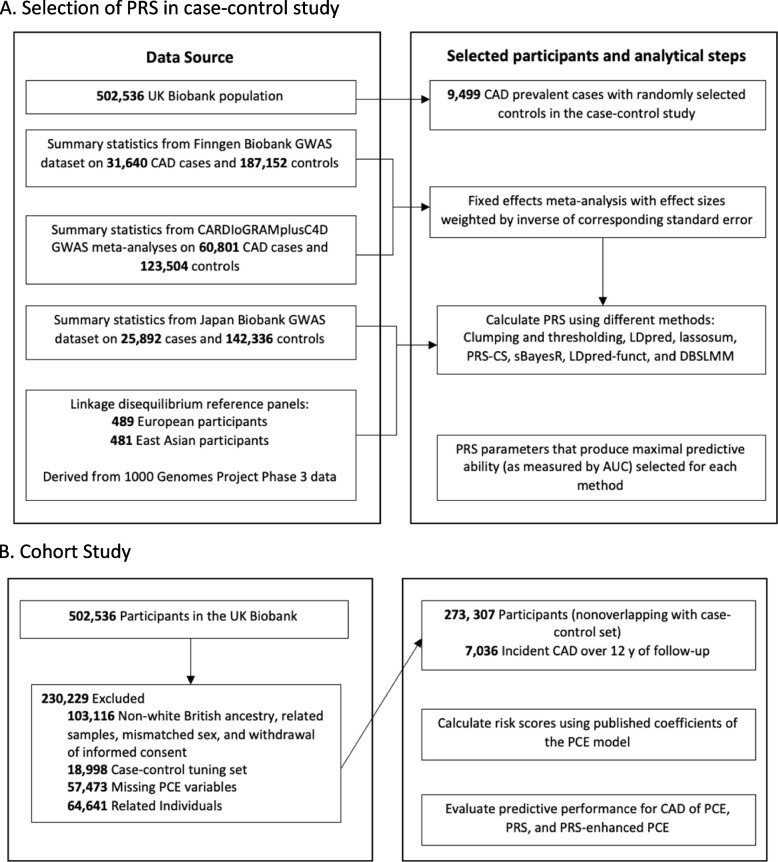
The value of polygenic risk scores (PRSs) towards improving guideline-recommended clinical risk models for coronary artery disease (CAD) prediction is controversial. Here we examine whether an integrated polygenic risk score improves the prediction of CAD beyond pooled cohort equations. METHODS: An observation study of 291,305 unrelated White British UK Biobank participants enrolled from 2006 to 2010 was conducted. A case-control sample of 9499 prevalent CAD cases and an equal number of randomly selected controls was used for tuning and integrating of the polygenic risk scores. A separate cohort of 272,307 individuals (with follow-up to 2020) was used to examine the risk prediction performance of pooled cohort equations, integrated polygenic risk score, and PRS-enhanced pooled cohort equation for incident CAD cases. The performance of each model was analyzed by discrimination and risk reclassification using a 7.5% threshold.
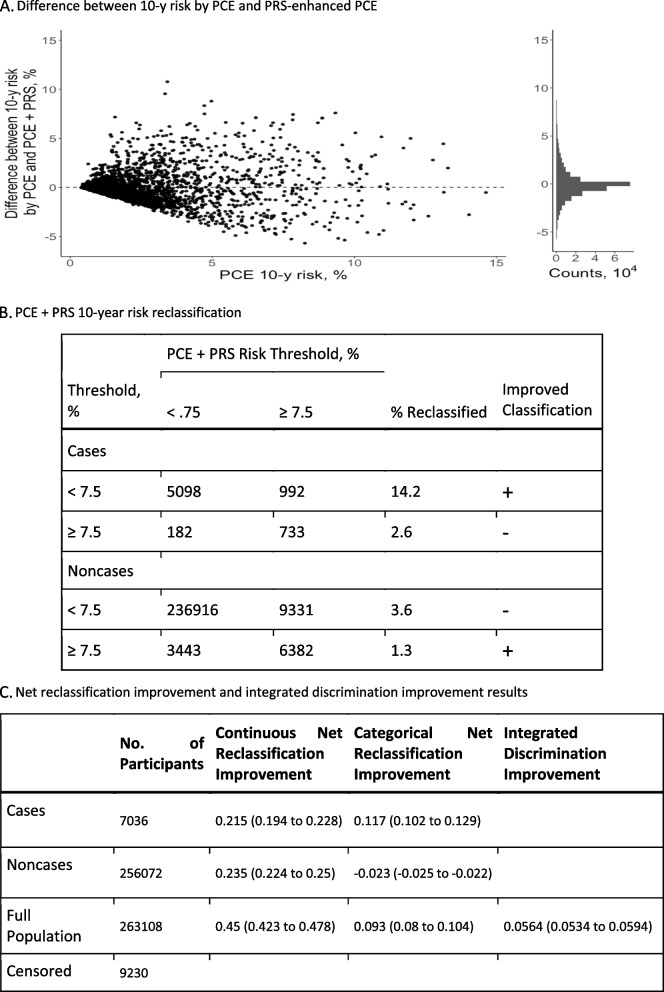
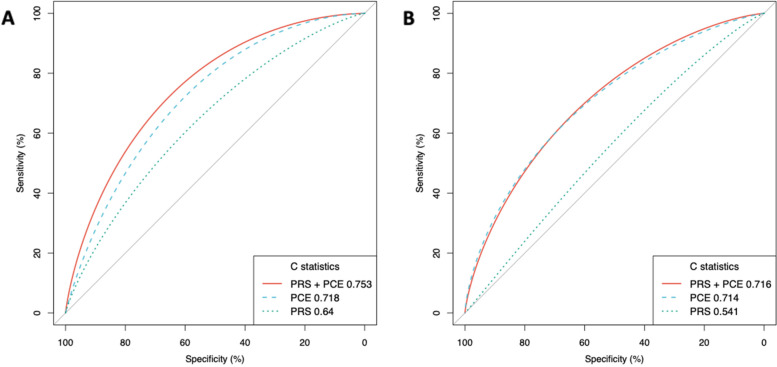
In the cohort of 272,307 individuals (mean age, 56.7 years) used to analyze predictive accuracy, there were 7036 incident CAD cases over a 12-year follow-up period. Model discrimination was tested for integrated polygenic risk score, pooled cohort equation, and PRS-enhanced pooled cohort equation with reported C-statistics of 0.640 (95% CI, 0.634-0.646), 0.718 (95% CI, 0.713-0.723), and 0.753 (95% CI, 0.748-0.758), respectively. Risk reclassification for the addition of the integrated polygenic risk score to the pooled cohort equation at a 7.5% risk threshold resulted in a net reclassification improvement of 0.117 (95% CI, 0.102 to 0.129) for cases and - 0.023 (95% CI, - 0.025 to - 0.022) for noncases [overall: 0.093 (95% CI, 0.08 to 0.104)]. For incident CAD cases, this represented 14.2% correctly reclassified to the higher-risk category and 2.6% incorrectly reclassified to the lower-risk category.
Addition of the integrated polygenic risk score for CAD to the pooled cohort questions improves the predictive accuracy for incident CAD and clinical risk classification in the White British from the UK Biobank. These findings suggest that an integrated polygenic risk score may enhance CAD risk prediction and screening in the White British population.
多基因风险评分(PRSs)对改善冠心病(CAD)预测的推荐临床风险模型的价值存在争议。在这里,我们研究了综合多基因风险评分是否可以提高 CAD 的预测能力,超越汇总队列方程。
对 2006 年至 2010 年期间招募的 291305 名无亲缘关系的白种英国生物库参与者进行了一项观察性研究。使用 9499 例现患 CAD 病例和相同数量的随机选择的对照病例的病例对照样本,对多基因风险评分进行调整和整合。使用 272307 名个体(随访至 2020 年)的单独队列来检查汇总队列方程、综合多基因风险评分和 PRS 增强型汇总队列方程对新发 CAD 病例的风险预测性能。使用 7.5%的阈值分析了每个模型的判别和风险再分类的性能。
在用于分析预测准确性的 272307 名个体(平均年龄 56.7 岁)的队列中,在 12 年的随访期间发生了 7036 例新发 CAD 病例。分别报告了综合多基因风险评分、汇总队列方程和 PRS 增强型汇总队列方程的模型判别能力,其 C 统计量分别为 0.640(95%CI,0.634-0.646)、0.718(95%CI,0.713-0.723)和 0.753(95%CI,0.748-0.758)。在 7.5%风险阈值下,将综合多基因风险评分添加到汇总队列方程中,对病例的净再分类改善为 0.117(95%CI,0.102-0.129),对非病例的改善为-0.023(95%CI,-0.025-0.022)[总体:0.093(95%CI,0.08-0.104)]。对于新发 CAD 病例,这代表 14.2%的病例被正确地重新分类为高危类别,2.6%的病例被错误地重新分类为低危类别。
将 CAD 的综合多基因风险评分添加到汇总队列问题中,可以提高白种英国人的 CAD 预测准确性和临床风险分类。这些发现表明,综合多基因风险评分可能会增强白种英国人的 CAD 风险预测和筛查。