College of Engineering, Tunghai University, Taichung, Taiwan.
Artificial Intelligence Center, Tunghai University, Taichung, Taiwan.
BMC Anesthesiol. 2022 Nov 14;22(1):351. doi: 10.1186/s12871-022-01888-y.
Weaning from mechanical ventilation (MV) is an essential issue in critically ill patients, and we used an explainable machine learning (ML) approach to establish an extubation prediction model.
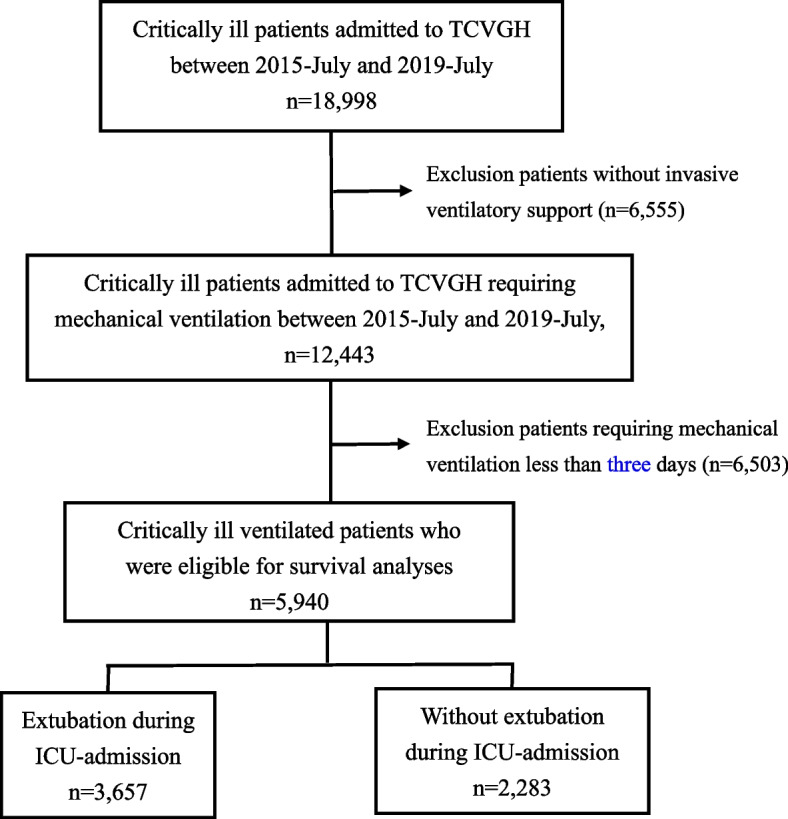
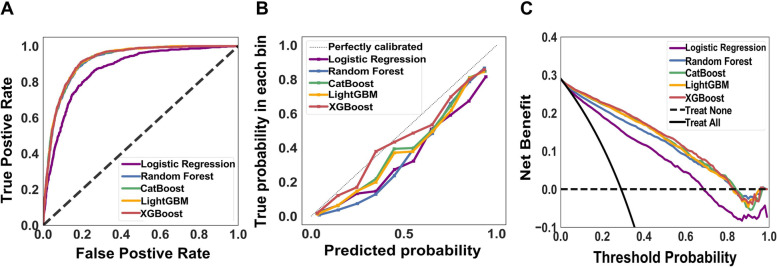
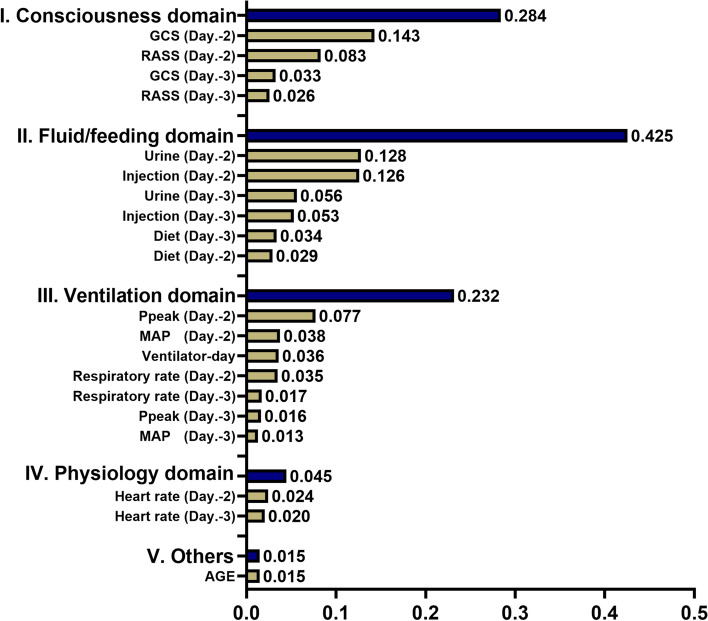
We enrolled patients who were admitted to intensive care units during 2015-2019 at Taichung Veterans General Hospital, a referral hospital in central Taiwan. We used five ML models, including extreme gradient boosting (XGBoost), categorical boosting (CatBoost), light gradient boosting machine (LightGBM), random forest (RF) and logistic regression (LR), to establish the extubation prediction model, and the feature window as well as prediction window was 48 h and 24 h, respectively. We further employed feature importance, Shapley additive explanations (SHAP) plot, partial dependence plot (PDP) and local interpretable model-agnostic explanations (LIME) for interpretation of the model at the domain, feature, and individual levels.
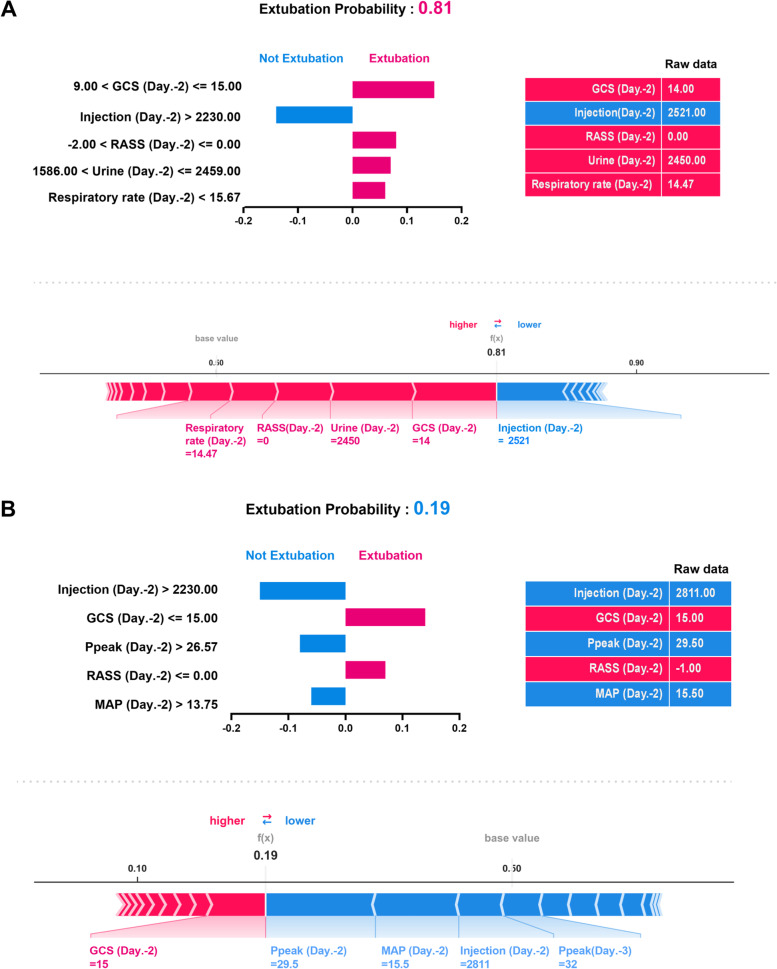
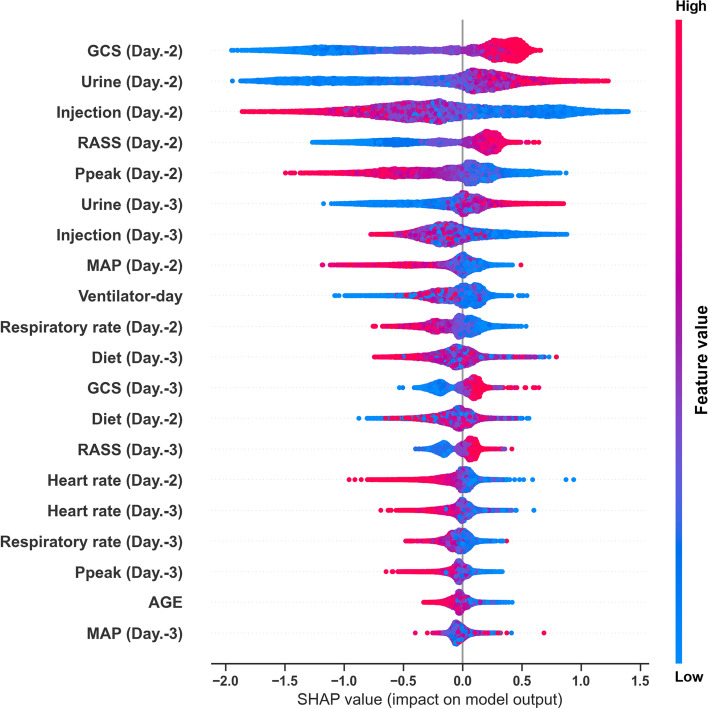
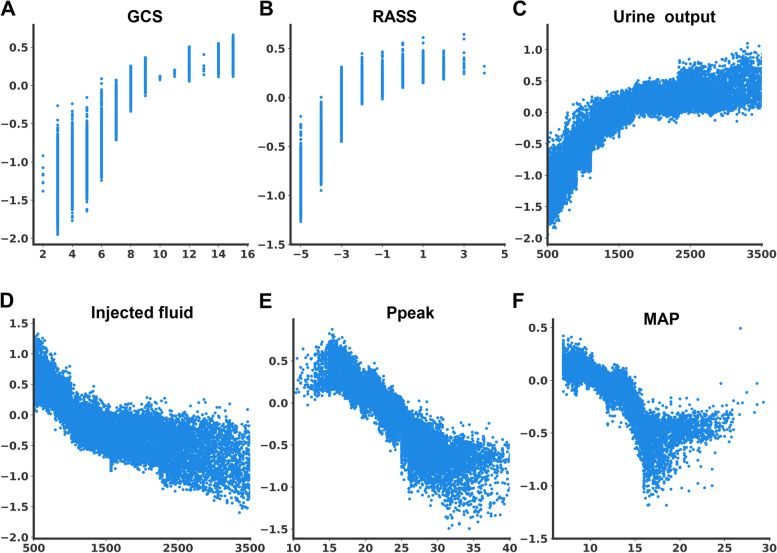
We enrolled 5,940 patients and found the accuracy was comparable among XGBoost, LightGBM, CatBoost and RF, with the area under the receiver operating characteristic curve using XGBoost to predict extubation was 0.921. The calibration and decision curve analysis showed well applicability of models. We also used the SHAP summary plot and PDP plot to demonstrate discriminative points of six key features in predicting extubation. Moreover, we employed LIME and SHAP force plots to show predicted probabilities of extubation and the rationale of the prediction at the individual level.
We developed an extubation prediction model with high accuracy and visualised explanations aligned with clinical workflow, and the model may serve as an autonomous screen tool for timely weaning.
机械通气(MV)撤机是危重症患者的一个重要问题,我们采用可解释的机器学习(ML)方法来建立拔管预测模型。
我们纳入了 2015 年至 2019 年期间在台湾中部转诊医院台中荣民总医院重症监护病房住院的患者。我们使用了五种 ML 模型,包括极端梯度提升(XGBoost)、分类梯度提升(CatBoost)、轻梯度提升机(LightGBM)、随机森林(RF)和逻辑回归(LR),来建立拔管预测模型,特征窗口和预测窗口分别为 48 小时和 24 小时。我们进一步在域、特征和个体层面上使用特征重要性、Shapley 加性解释(SHAP)图、部分依赖图(PDP)和局部可解释模型不可知解释(LIME)对模型进行解释。
我们共纳入了 5940 名患者,发现 XGBoost、LightGBM、CatBoost 和 RF 的准确率相当,XGBoost 预测拔管的受试者工作特征曲线下面积为 0.921。校准和决策曲线分析表明模型具有良好的适用性。我们还使用 SHAP 总结图和 PDP 图展示了在预测拔管中六个关键特征的区分点。此外,我们采用 LIME 和 SHAP 力图展示了在个体水平上的拔管预测概率和预测依据。
我们开发了一种具有高准确率的拔管预测模型,并提供了与临床工作流程一致的可视化解释,该模型可以作为一种自主的拔管筛查工具。