Zhao Qin-Yu, Wang Huan, Luo Jing-Chao, Luo Ming-Hao, Liu Le-Ping, Yu Shen-Ji, Liu Kai, Zhang Yi-Jie, Sun Peng, Tu Guo-Wei, Luo Zhe
College of Engineering and Computer Science, Australian National University, Canberra, ACT, Australia.
Department of Critical Care Medicine, Zhongshan Hospital, Fudan University, Shanghai, China.
Front Med (Lausanne). 2021 May 17;8:676343. doi: 10.3389/fmed.2021.676343. eCollection 2021.
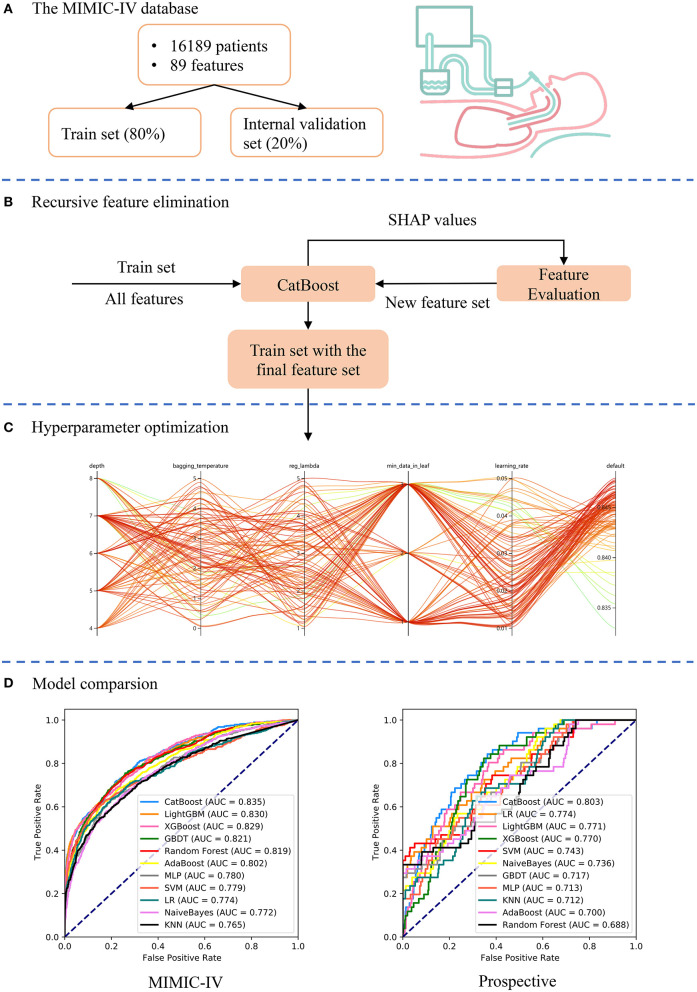
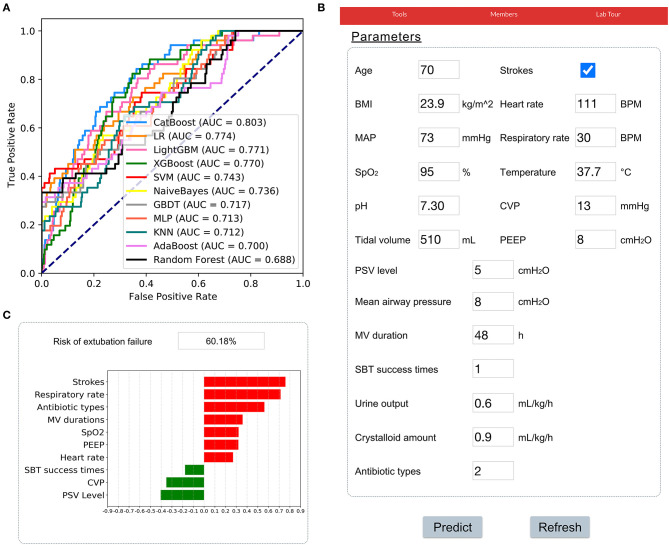
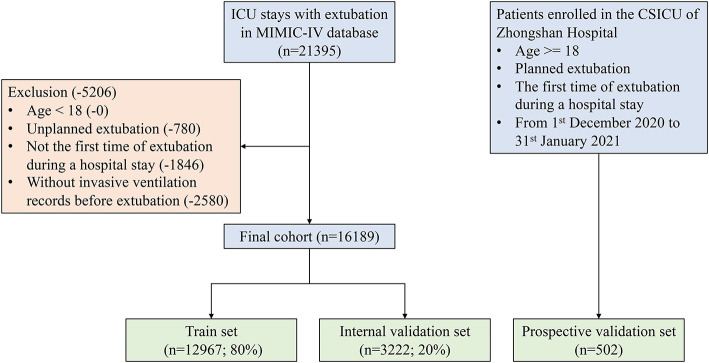
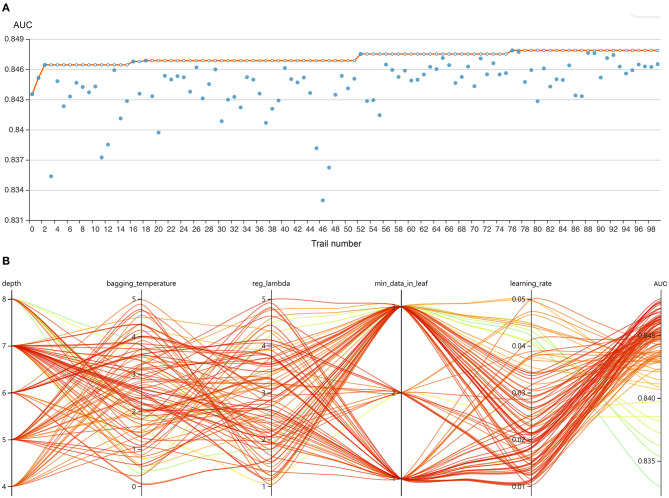
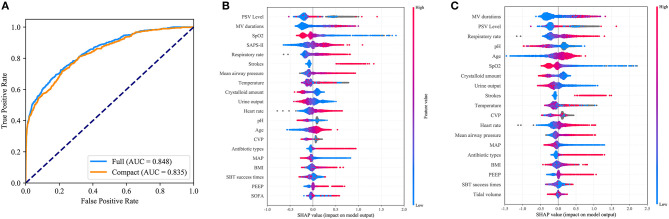
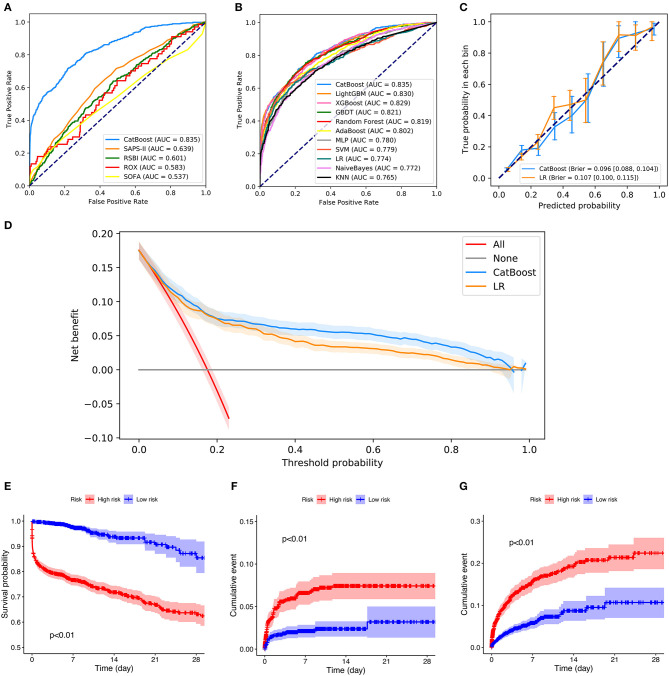
Extubation failure (EF) can lead to an increased chance of ventilator-associated pneumonia, longer hospital stays, and a higher mortality rate. This study aimed to develop and validate an accurate machine-learning model to predict EF in intensive care units (ICUs). Patients who underwent extubation in the Medical Information Mart for Intensive Care (MIMIC)-IV database were included. EF was defined as the need for ventilatory support (non-invasive ventilation or reintubation) or death within 48 h following extubation. A machine-learning model called Categorical Boosting (CatBoost) was developed based on 89 clinical and laboratory variables. SHapley Additive exPlanations (SHAP) values were calculated to evaluate feature importance and the recursive feature elimination (RFE) algorithm was used to select key features. Hyperparameter optimization was conducted using an automated machine-learning toolkit (Neural Network Intelligence). The final model was trained based on key features and compared with 10 other models. The model was then prospectively validated in patients enrolled in the Cardiac Surgical ICU of Zhongshan Hospital, Fudan University. In addition, a web-based tool was developed to help clinicians use our model. Of 16,189 patients included in the MIMIC-IV cohort, 2,756 (17.0%) had EF. Nineteen key features were selected using the RFE algorithm, including age, body mass index, stroke, heart rate, respiratory rate, mean arterial pressure, peripheral oxygen saturation, temperature, pH, central venous pressure, tidal volume, positive end-expiratory pressure, mean airway pressure, pressure support ventilation (PSV) level, mechanical ventilation (MV) durations, spontaneous breathing trial success times, urine output, crystalloid amount, and antibiotic types. After hyperparameter optimization, our model had the greatest area under the receiver operating characteristic (AUROC: 0.835) in internal validation. Significant differences in mortality, reintubation rates, and NIV rates were shown between patients with a high predicted risk and those with a low predicted risk. In the prospective validation, the superiority of our model was also observed (AUROC: 0.803). According to the SHAP values, MV duration and PSV level were the most important features for prediction. In conclusion, this study developed and prospectively validated a CatBoost model, which better predicted EF in ICUs than other models.
拔管失败(EF)会增加呼吸机相关性肺炎的发生几率、延长住院时间并提高死亡率。本研究旨在开发并验证一种准确的机器学习模型,以预测重症监护病房(ICU)中的拔管失败情况。纳入了在重症监护医学信息数据库(MIMIC-IV)中接受拔管的患者。拔管失败定义为拔管后48小时内需要通气支持(无创通气或重新插管)或死亡。基于89个临床和实验室变量开发了一种名为分类提升(CatBoost)的机器学习模型。计算了SHapley加性解释(SHAP)值以评估特征重要性,并使用递归特征消除(RFE)算法选择关键特征。使用自动化机器学习工具包(神经网络智能)进行超参数优化。最终模型基于关键特征进行训练,并与其他10种模型进行比较。然后在复旦大学附属中山医院心脏外科ICU登记的患者中对该模型进行前瞻性验证。此外,还开发了一个基于网络的工具,以帮助临床医生使用我们的模型。在MIMIC-IV队列纳入的16189例患者中,2756例(17.0%)发生了拔管失败。使用RFE算法选择了19个关键特征,包括年龄、体重指数、中风、心率、呼吸频率、平均动脉压、外周血氧饱和度、体温、pH值、中心静脉压、潮气量、呼气末正压、平均气道压、压力支持通气(PSV)水平、机械通气(MV)持续时间、自主呼吸试验成功次数、尿量、晶体液量和抗生素类型。经过超参数优化后,我们的模型在内部验证中的受试者操作特征曲线下面积最大(曲线下面积:0.835)。预测风险高的患者与预测风险低的患者在死亡率、重新插管率和无创通气率方面存在显著差异。在前瞻性验证中,也观察到了我们模型的优越性(曲线下面积:0.803)。根据SHAP值,MV持续时间和PSV水平是预测的最重要特征。总之,本研究开发并前瞻性验证了一种CatBoost模型,该模型在ICU中比其他模型能更好地预测拔管失败情况。