Amano Koji, Koshimoto Saori, Hopkinson Jane B, Baracos Vickie E, Mori Naoharu, Morita Tatsuya, Oyamada Shunsuke, Ishiki Hiroto, Satomi Eriko, Takeuchi Takashi
Department of Palliative Medicine, National Cancer Center Hospital, Tokyo, Japan.
Department of Palliative and Supportive Medicine, Graduate School of Medicine, Aichi Medical University, Aichi, Japan.
Palliat Med Rep. 2022 Dec 2;3(1):244-254. doi: 10.1089/pmr.2022.0045. eCollection 2022.
Holistic multimodal interventions have not been established for cancer cachexia. The beliefs and perceptions of health care professionals (HCPs) based on their experiences influence the interventions.
HCPs' knowledge, perceptions, and practices in cancer cachexia management were evaluated.
DESIGN/SETTING/SUBJECTS/MEASUREMENTS: A nationwide questionnaire survey was conducted that focused on the perspectives of HCPs on interventions in 451 designated cancer hospitals across Japan. Descriptive statistics were applied.
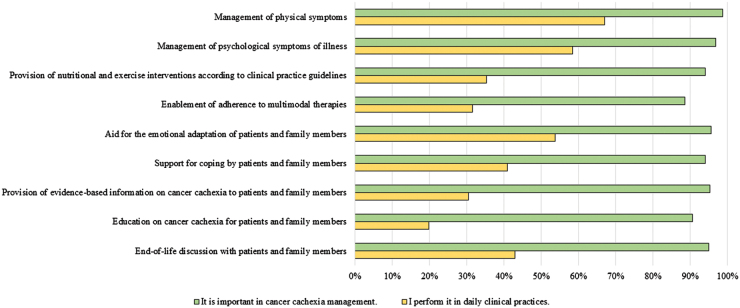
Among 2255 participants, 1320 responded (58.5%), and 1188 in 258 institutes were included in the analysis. The current international definition of cancer cachexia is not commonly known and recent clinical practice guidelines have not been widely adopted. More than 50% of participants considered ≥5% weight loss in six months and ECOG PS (Eastern Cooperative Oncology Group Performance Status) 2-4 to be cancer cachexia, whereas 50% answered that there was no relationship between life expectancy and cancer cachexia. Participants tended to consider it important to initiate nutritional and exercise interventions before cancer cachexia becomes apparent. The majority of participants recognized the importance of holistic multimodal interventions, particularly for the management of physical and psychological symptoms; however, only 20% reported that they educated patients and families. Furthermore, 33% of participants considered themselves to have provided patients and families with sufficient nutritional and exercise interventions and evidence-based information.
The results reveal that HCPs are not regularly providing education and emotional support to patients and families suffering from cancer cachexia. The results also show the need for education for HCPs to enhance implementation of holistic multimodal interventions for cancer cachexia.
尚未建立针对癌症恶病质的整体多模式干预措施。医护人员基于自身经验形成的信念和认知会影响干预措施。
评估医护人员在癌症恶病质管理方面的知识、认知和实践。
设计/地点/受试者/测量方法:开展了一项全国性问卷调查,重点关注日本451家指定癌症医院中医护人员对干预措施的看法。应用描述性统计方法。
在2255名参与者中,1320人做出回应(58.5%),258家机构的1188人纳入分析。目前癌症恶病质的国际定义并不广为人知,近期的临床实践指南也未得到广泛采用。超过50%的参与者认为六个月内体重减轻≥5%以及东部肿瘤协作组体能状态(ECOG PS)为2 - 4级属于癌症恶病质,而50%的人回答预期寿命与癌症恶病质之间没有关系。参与者倾向于认为在癌症恶病质明显出现之前启动营养和运动干预很重要。大多数参与者认识到整体多模式干预的重要性,特别是对于身体和心理症状的管理;然而,只有20%的人报告称他们对患者及其家属进行了教育。此外,33%的参与者认为自己为患者及其家属提供了足够的营养和运动干预以及循证信息。
结果显示,医护人员并未定期为患有癌症恶病质的患者及其家属提供教育和情感支持。结果还表明需要对医护人员进行教育,以加强对癌症恶病质的整体多模式干预措施的实施。