Department of Orthopaedic, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand.
Center of Excellence in Biomechanics and Innovative Spine Surgery, Chulalongkorn University, Bangkok, Thailand.
Eur Spine J. 2023 Aug;32(8):2736-2747. doi: 10.1007/s00586-023-07678-5. Epub 2023 Apr 3.
We aimed to demonstrate non-inferiority in terms of functional outcomes in patients with lumbar spinal stenosis who underwent full-endoscopic decompression compared with tubular-based microscopic decompression.
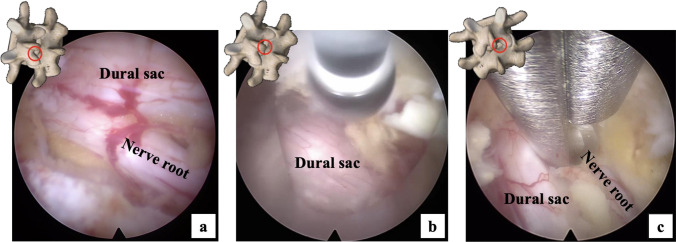
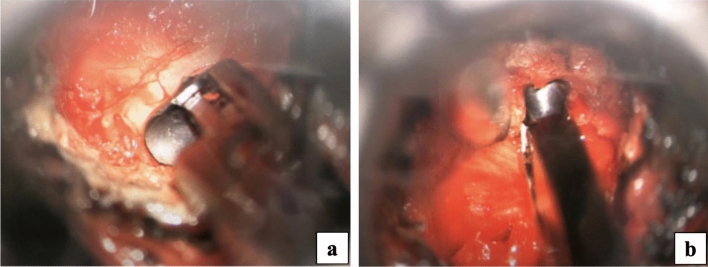
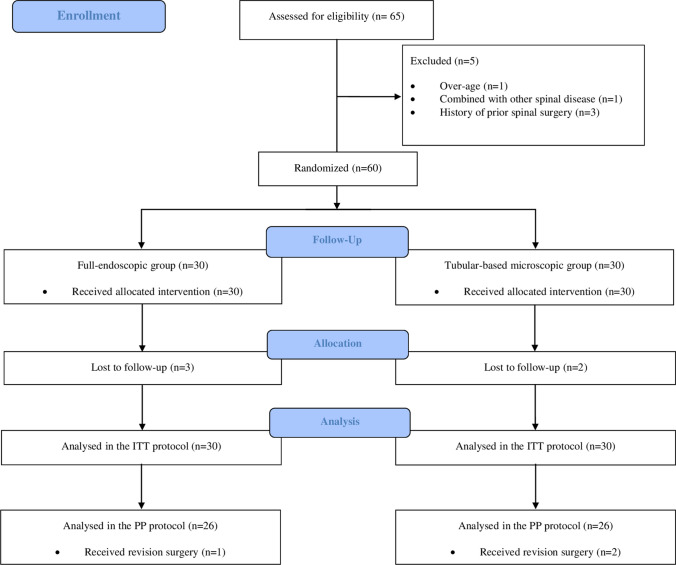
This prospective, randomized controlled, non-inferiority trial included 60 patients with single-level lumbar spinal stenosis who required decompression surgery. The patients were randomly assigned in a 1:1 ratio to the full-endoscopic group (FE group) or the tubular-based microscopic group (TM group). Based on intention-to-treat analysis, the primary outcome was the Oswestry Disability Index score at 24 months postoperative. The secondary outcomes included the visual analog scale (VAS) score for back and leg pain, European Quality of Life-5 Dimensions (EQ-5D) score, walking time, and patient satisfaction rate according to the modified MacNab criteria. Surgery-related outcomes were also analyzed.
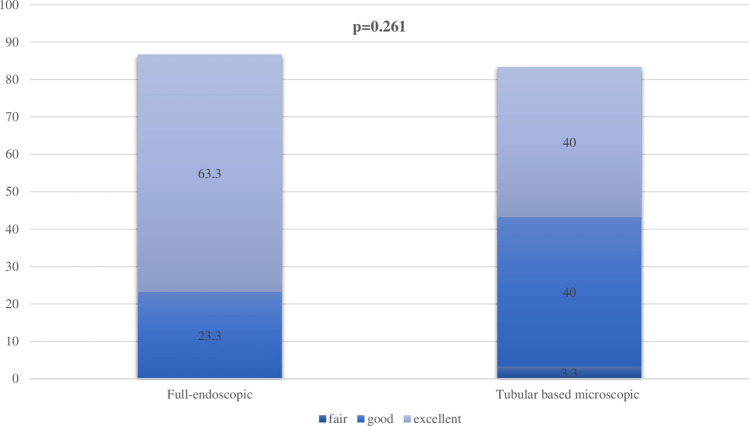
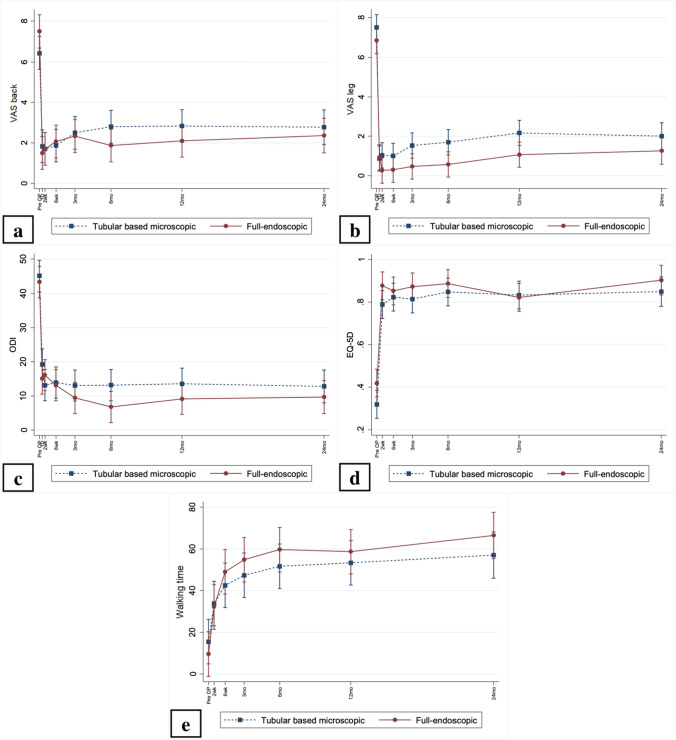
Of the total patients, 92% (n = 55) completed a 24-month follow-up. The primary outcomes were comparable between the two groups (p = 0.748). However, the FE group showed a statistically significant improvement in the mean VAS score for back pain at day 1 and at 6, 12, and 24 months after surgery (p < 0.05). No significant difference was observed in the VAS score for leg pain, EQ-5D score, or walking time (p > 0.05). Regarding the modified MacNab criteria, 86.7% of patients in the FE group and 83.3% in the TM group had excellent or good results at 24 months after surgery (p = 0.261). Despite the similar results in surgery-related outcomes, including operative time, radiation exposure, revision rate, and complication rate, between the two groups (p > 0.05), less blood loss and shorter length of hospital stay were observed in the FE group (p ≤ 0.001 and 0.011, respectively).
This study suggests that full-endoscopic decompression is an alternative treatment for patients with lumbar spinal stenosis because it provides non-inferior clinical efficacy and safety compared with tubular-based microscopic surgery. In addition, it offers advantages in terms of less invasive surgery. Trial registration number (TRN): TCTR20191217001.
我们旨在证明与基于管的显微镜减压相比,全内窥镜减压治疗腰椎管狭窄症患者在功能结局方面具有非劣效性。
这是一项前瞻性、随机对照、非劣效性试验,纳入了 60 例需要减压手术的单节段腰椎管狭窄症患者。患者按照 1:1 的比例随机分为全内窥镜组(FE 组)或基于管的显微镜组(TM 组)。根据意向治疗分析,主要结局是术后 24 个月的 Oswestry 功能障碍指数评分。次要结局包括腰背疼痛的视觉模拟量表(VAS)评分、欧洲生活质量-5 维度(EQ-5D)评分、行走时间以及根据改良 MacNab 标准的患者满意度。还分析了手术相关结局。
在所有患者中,92%(n=55)完成了 24 个月的随访。两组的主要结局相当(p=0.748)。然而,FE 组在术后第 1 天以及术后 6、12 和 24 个月时的腰背疼痛 VAS 评分均有显著改善(p<0.05)。下肢疼痛 VAS 评分、EQ-5D 评分或行走时间无显著差异(p>0.05)。根据改良 MacNab 标准,FE 组和 TM 组分别有 86.7%和 83.3%的患者在术后 24 个月时获得了优秀或良好的结果(p=0.261)。尽管两组在手术相关结局(包括手术时间、辐射暴露、翻修率和并发症率)方面相似(p>0.05),但 FE 组的出血量更少,住院时间更短(p≤0.001 和 0.011)。
本研究表明,全内窥镜减压是治疗腰椎管狭窄症的一种替代治疗方法,因为与基于管的显微镜手术相比,它具有非劣效的临床疗效和安全性。此外,它在微创手术方面具有优势。试验注册号(TRN):TCTR20191217001。