CARTaGENE (Jantzen, Broët), Research Centre, CHU Sainte-Justine; Université de Montréal (Jantzen, Broët); Département de médecine sociale et préventive (Broët), École de santé publique de l'Université de Montréal, Université de Montréal; Departments of Medicine (Ezer) and of Pathology (Camilleri-Broët), McGill University, Montréal, Que.; Prevention and Cancer Control (Tammemägi), Ontario Health (Cancer Care Ontario), Toronto, Ont.; Department of Health Sciences (Tammemägi), Brock University, St. Catharines, Ont.; Department of Public Health (Broët), Faculty of Medicine; Centre de recherche en epidémiologie et santé des populations and INSERM (Broët), Université Paris-Saclay; Assistance Publique-Hôpitaux de Paris (Broët), Hôpitaux Universitaires Paris-Sud, Hôpital Paul Brousse, Villejuif, France
CARTaGENE (Jantzen, Broët), Research Centre, CHU Sainte-Justine; Université de Montréal (Jantzen, Broët); Département de médecine sociale et préventive (Broët), École de santé publique de l'Université de Montréal, Université de Montréal; Departments of Medicine (Ezer) and of Pathology (Camilleri-Broët), McGill University, Montréal, Que.; Prevention and Cancer Control (Tammemägi), Ontario Health (Cancer Care Ontario), Toronto, Ont.; Department of Health Sciences (Tammemägi), Brock University, St. Catharines, Ont.; Department of Public Health (Broët), Faculty of Medicine; Centre de recherche en epidémiologie et santé des populations and INSERM (Broët), Université Paris-Saclay; Assistance Publique-Hôpitaux de Paris (Broët), Hôpitaux Universitaires Paris-Sud, Hôpital Paul Brousse, Villejuif, France.
CMAJ Open. 2023 Apr 11;11(2):E314-E322. doi: 10.9778/cmajo.20210335. Print 2023 Mar-Apr.
The PLCO prediction tool for risk of lung cancer has been proposed for a pilot program for lung cancer screening in Quebec, but has not been validated in this population. We sought to validate PLCO in a cohort of Quebec residents, and to determine the hypothetical performance of different screening strategies.
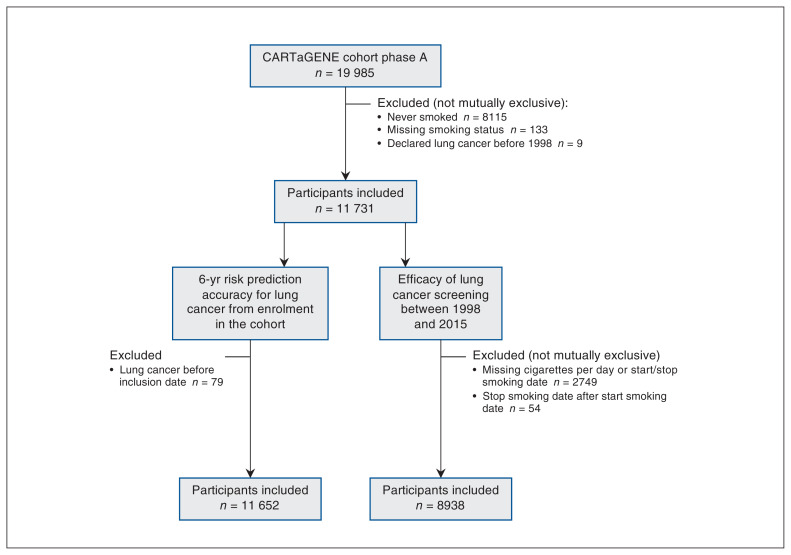
We included smokers without a history of lung cancer from the population-based CARTaGENE cohort. To assess PLCO calibration and discrimination, we determined the ratio of expected to observed number of cases, as well as the sensitivity, specificity and positive predictive values of different risk thresholds. To assess the performance of screening strategies if applied between Jan. 1, 1998, and Dec. 31, 2015, we tested different thresholds of the PLCO detection of lung cancer over 6 years (1.51%, 1.70% and 2.00%), the criteria of Quebec's pilot program (for people aged 55-74 yr and 50-74 yr) and recommendations from 2021 United States and 2016 Canada guidelines. We assessed shift and serial scenarios of screening, whereby eligibility was assessed annually or every 6 years, respectively.
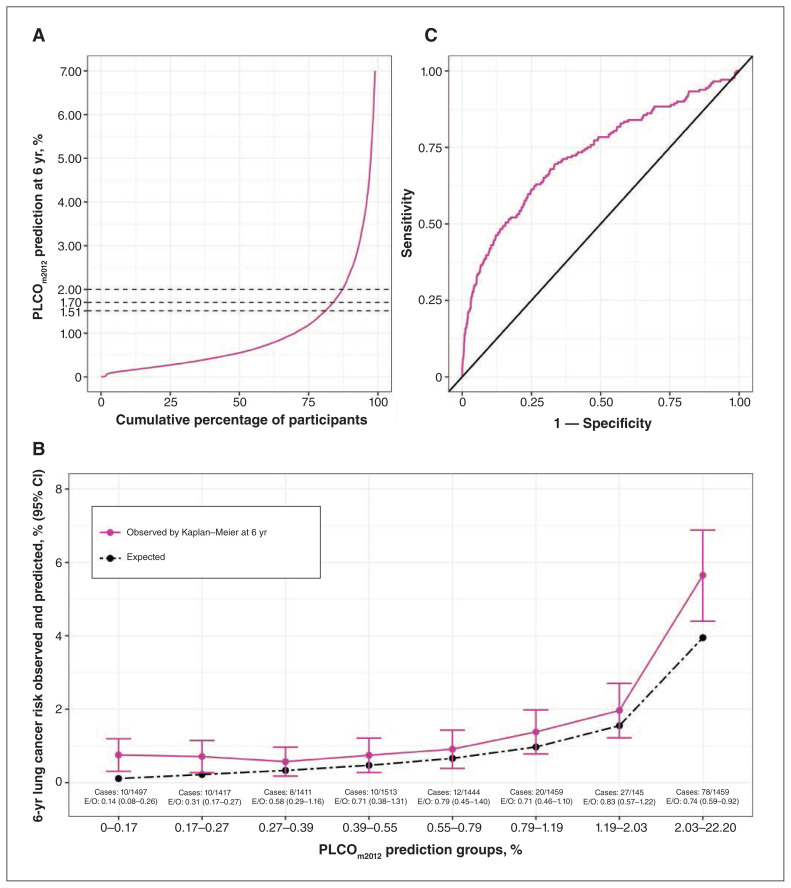
Among 11 652 participants, 176 (1.51%) lung cancers were diagnosed in 6 years. The PLCO tool underestimated the number of cases (expected-to-observed ratio 0.68, 95% confidence interval [CI] 0.59-0.79), but the discrimination was good (C-statistic 0.727, 95% CI 0.679-0.770). From a threshold of 1.51% to 2.00%, sensitivities ranged from 52.3% (95% CI 44.6%-59.8%) to 44.9% (95% CI 37.4%-52.6%), specificities ranged from 81.6% (95% CI 80.8%-82.3%) to 87.7% (95% CI 87.0%-88.3%) and positive predictive values ranged from 4.2% (95% CI 3.4%-5.1%) to 5.3% (95% CI 4.2%-6.5%). Overall, 8938 participants had sufficient data to test performance of screening strategies. If eligibility was estimated annually, Quebec pilot criteria would have detected fewer cancers than PLCO at a 2.00% threshold (48.3% v. 50.2%) for a similar number of scans per detected cancer. If eligibility was estimated every 6 years, up to 26 fewer lung cancers would have been detected; however, this scenario led to higher positive predictive values (highest for PLCO with a 2.00% threshold at 6.0%, 95% CI 4.8%-7.3%).
In a cohort of Quebec smokers, the PLCO risk prediction tool had good discrimination in detecting lung cancer, but it may be helpful to adjust the intercept to improve calibration. The implementation of risk prediction models in some of the provinces of Canada should be done with caution.
PLCO 预测工具被提出用于魁北克的肺癌筛查试点项目,但尚未在该人群中进行验证。我们旨在对魁北克居民队列中的 PLCO 进行验证,并确定不同筛查策略的假设性能。
我们纳入了来自基于人群的 CARTaGENE 队列中无肺癌病史的吸烟者。为了评估 PLCO 的校准和判别能力,我们确定了预期病例数与实际病例数的比值,以及不同风险阈值的灵敏度、特异性和阳性预测值。为了评估如果在 1998 年 1 月 1 日至 2015 年 12 月 31 日期间应用筛查策略的性能,我们测试了 PLCO 检测肺癌的不同阈值(6 年为 1.51%、1.70%和 2.00%)、魁北克试点计划的标准(55-74 岁和 50-74 岁的人群)以及 2021 年美国和 2016 年加拿大指南的建议。我们评估了筛查的转移和连续方案,分别每年或每 6 年评估一次资格。
在 11652 名参与者中,6 年内诊断出 176 例(1.51%)肺癌。PLCO 工具低估了病例数(预期与观察到的病例数之比为 0.68,95%置信区间[CI]为 0.59-0.79),但判别能力良好(C 统计量为 0.727,95%CI 为 0.679-0.770)。从 1.51%到 2.00%的阈值,灵敏度范围为 52.3%(95%CI 为 44.6%-59.8%)到 44.9%(95%CI 为 37.4%-52.6%),特异性范围为 81.6%(95%CI 为 80.8%-82.3%)到 87.7%(95%CI 为 87.0%-88.3%),阳性预测值范围为 4.2%(95%CI 为 3.4%-5.1%)到 5.3%(95%CI 为 4.2%-6.5%)。总体而言,8938 名参与者有足够的数据来测试筛查策略的性能。如果每年估计资格,与 PLCO 相比,魁北克试点标准在 2.00%的阈值下(48.3%比 50.2%)检测到的癌症数量较少,为每检测到一个癌症进行的扫描数量相似。如果每 6 年估计一次资格,将检测到的肺癌病例数减少 26 例;然而,这种情况导致阳性预测值更高(PLCO 的最高值为 6.0%,95%CI 为 4.8%-7.3%)。
在魁北克吸烟者队列中,PLCO 风险预测工具在检测肺癌方面具有良好的判别能力,但可能需要调整截距以提高校准度。加拿大一些省份实施风险预测模型应谨慎。