School of Public Health, Imperial College London, London, United Kingdom.
MRC Centre for Global infectious Disease Analysis and Abdul Latif Jameel Institute for Disease and Emergency Analytics, Imperial College London, London, United Kingdom.
PLoS Biol. 2023 May 25;21(5):e3002118. doi: 10.1371/journal.pbio.3002118. eCollection 2023 May.
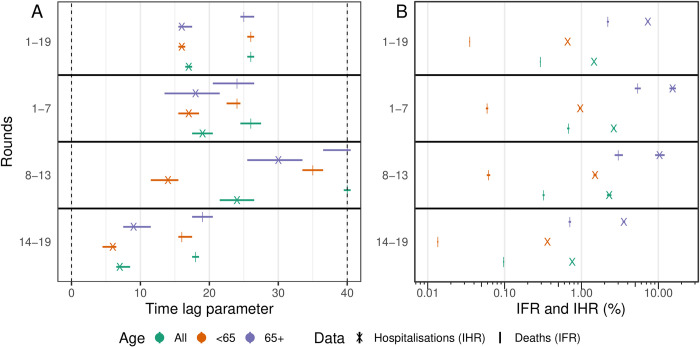
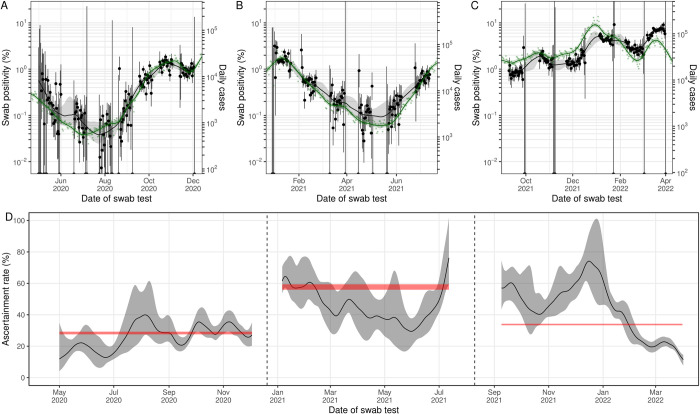
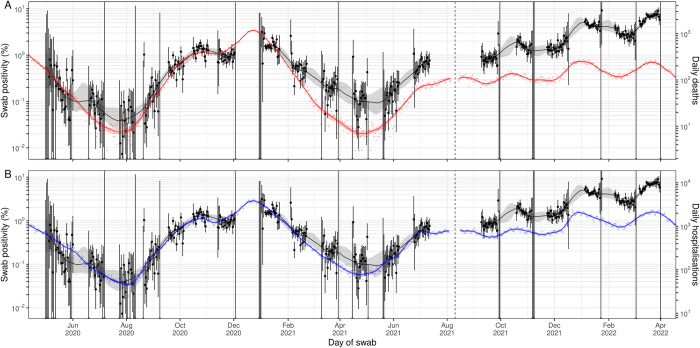
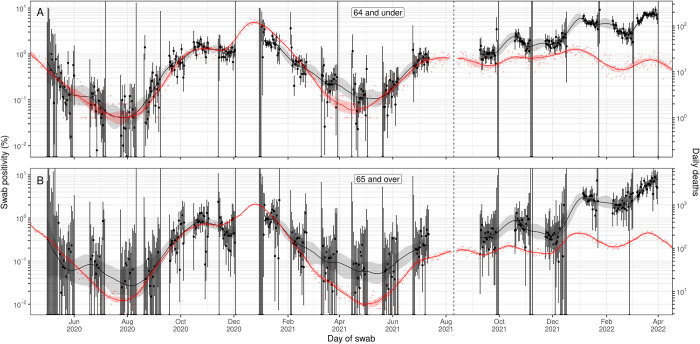
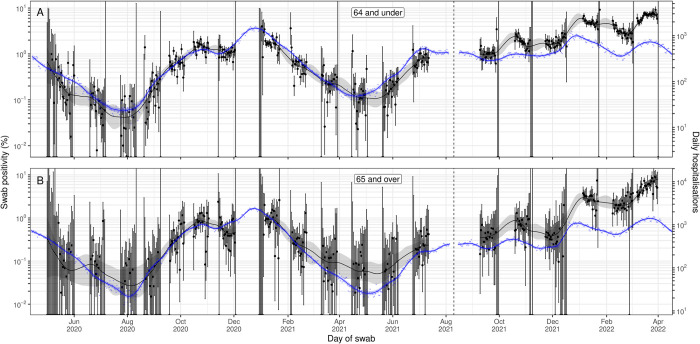
The relationship between prevalence of infection and severe outcomes such as hospitalisation and death changed over the course of the COVID-19 pandemic. Reliable estimates of the infection fatality ratio (IFR) and infection hospitalisation ratio (IHR) along with the time-delay between infection and hospitalisation/death can inform forecasts of the numbers/timing of severe outcomes and allow healthcare services to better prepare for periods of increased demand. The REal-time Assessment of Community Transmission-1 (REACT-1) study estimated swab positivity for Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) infection in England approximately monthly from May 2020 to March 2022. Here, we analyse the changing relationship between prevalence of swab positivity and the IFR and IHR over this period in England, using publicly available data for the daily number of deaths and hospitalisations, REACT-1 swab positivity data, time-delay models, and Bayesian P-spline models. We analyse data for all age groups together, as well as in 2 subgroups: those aged 65 and over and those aged 64 and under. Additionally, we analysed the relationship between swab positivity and daily case numbers to estimate the case ascertainment rate of England's mass testing programme. During 2020, we estimated the IFR to be 0.67% and the IHR to be 2.6%. By late 2021/early 2022, the IFR and IHR had both decreased to 0.097% and 0.76%, respectively. The average case ascertainment rate over the entire duration of the study was estimated to be 36.1%, but there was some significant variation in continuous estimates of the case ascertainment rate. Continuous estimates of the IFR and IHR of the virus were observed to increase during the periods of Alpha and Delta's emergence. During periods of vaccination rollout, and the emergence of the Omicron variant, the IFR and IHR decreased. During 2020, we estimated a time-lag of 19 days between hospitalisation and swab positivity, and 26 days between deaths and swab positivity. By late 2021/early 2022, these time-lags had decreased to 7 days for hospitalisations and 18 days for deaths. Even though many populations have high levels of immunity to SARS-CoV-2 from vaccination and natural infection, waning of immunity and variant emergence will continue to be an upwards pressure on the IHR and IFR. As investments in community surveillance of SARS-CoV-2 infection are scaled back, alternative methods are required to accurately track the ever-changing relationship between infection, hospitalisation, and death and hence provide vital information for healthcare provision and utilisation.
在 COVID-19 大流行期间,感染的流行率与住院和死亡等严重后果之间的关系发生了变化。可靠的感染病死率 (IFR) 和感染住院率 (IHR) 估计值以及感染与住院/死亡之间的时间延迟,可以为严重后果的数量/时间预测提供信息,并使医疗保健服务能够更好地为需求增加的时期做好准备。REal-time Assessment of Community Transmission-1 (REACT-1) 研究大约每月从 2020 年 5 月到 2022 年 3 月在英格兰估计严重急性呼吸综合征冠状病毒 2 (SARS-CoV-2) 感染的拭子阳性率。在这里,我们使用公开的每日死亡和住院人数数据、REACT-1 拭子阳性数据、时间延迟模型和贝叶斯 P-样条模型,分析了在此期间英格兰拭子阳性率与 IFR 和 IHR 之间不断变化的关系。我们一起分析了所有年龄组的数据,以及两个亚组的数据:65 岁及以上组和 64 岁及以下组。此外,我们还分析了拭子阳性率与每日病例数之间的关系,以估计英格兰大规模检测计划的病例检出率。在 2020 年,我们估计 IFR 为 0.67%,IHR 为 2.6%。到 2021 年底/2022 年初,IFR 和 IHR 均下降至 0.097%和 0.76%。整个研究期间的平均病例检出率估计为 36.1%,但病例检出率的连续估计值存在一些显著差异。观察到病毒的 IFR 和 IHR 的连续估计值在 Alpha 和 Delta 出现期间增加。在疫苗接种推出期间和 Omicron 变体出现期间,IFR 和 IHR 下降。在 2020 年,我们估计住院和拭子阳性之间的时间延迟为 19 天,死亡和拭子阳性之间的时间延迟为 26 天。到 2021 年底/2022 年初,这些时间延迟分别减少到住院 7 天和死亡 18 天。尽管许多人群因接种疫苗和自然感染而对 SARS-CoV-2 具有高免疫力,但免疫力下降和变体出现仍将对 IHR 和 IFR 构成上行压力。随着对 SARS-CoV-2 感染的社区监测投资的减少,需要替代方法来准确跟踪感染、住院和死亡之间不断变化的关系,从而为医疗保健提供和利用提供重要信息。