Kreidieh Firas Y, Tawbi Hussein A
Department of Melanoma Medical Oncology, Division of Cancer Medicine, The University of Texas MD Anderson Cancer Center, Houston, TX, USA.
Department of Melanoma Medical Oncology, Division of Cancer Medicine, The University of Texas MD Anderson Cancer Center, 1515 Holcombe Blvd, Houston, TX 77030, USA.
Ther Adv Med Oncol. 2023 Jul 17;15:17588359231186027. doi: 10.1177/17588359231186027. eCollection 2023.
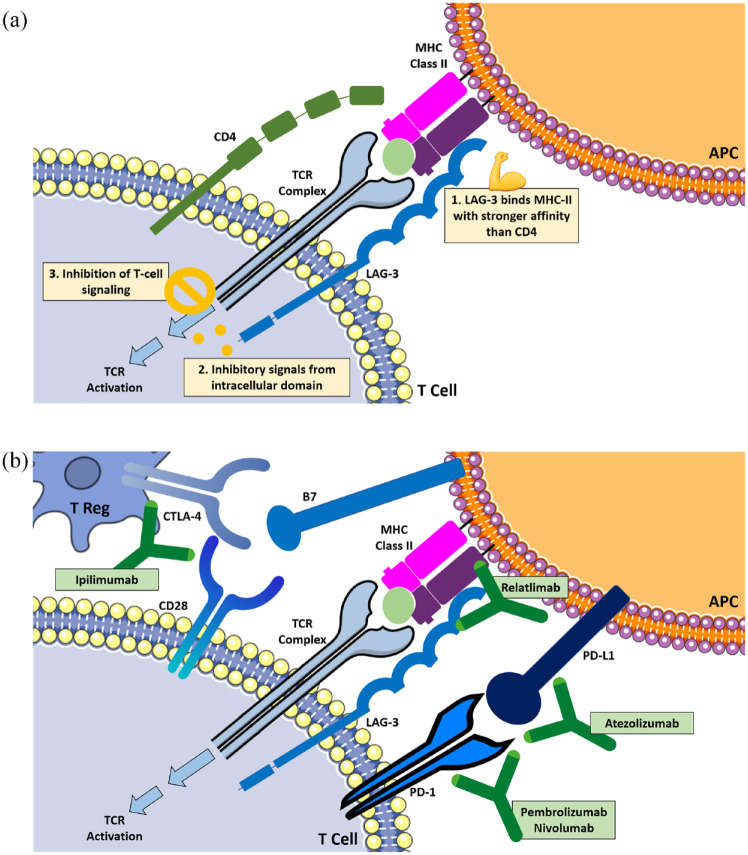
Despite major advances with immunotherapy and targeted therapy in the past decade, metastatic melanoma continues to be a deadly disease for close to half of all patients. Over the past decade, advancement in immune profiling and a deeper understanding of the immune tumor microenvironment (TME) have enabled the development of novel approaches targeting and a multitude of targets being investigated for the immunotherapy of melanoma. However, to date, immune checkpoint blockade has remained the most successful with programmed cell death-1 (PD-1)/programmed cell death ligand-1 (PD-L1) and cytotoxic T-lymphocyte antigen-4 (CTLA-4) inhibitors, alone or in combination, yielding the most robust and durable clinical outcome in patients with metastatic melanoma. The highest rate of durable responses is achieved with the combination with PD-1 and CTLA-4 inhibition, and is effective in a variety of settings including brain metastases; however, it comes at the expense of a multitude of life-threatening toxicities occurring in up to 60% of patients. This has also established melanoma as the forefront of immuno-oncology (IO) drug development, and the search for novel checkpoints has been ongoing with multiple relevant targets including T-cell immunoglobulin and mucinodomain containing-3 (TIM-3), LAG-3, V-domain immunoglobulin suppressor T-cell activation (VISTA), T-cell immunoglobulin and immunoreceptor tyrosine-based inhibitory motif (ITIM) domain (TIGIT), among others. Lymphocyte activation gene-3 (LAG-3), which is a co-inhibitory receptor on T cells that suppress their activation, has revolutionized immunomodulation in melanoma. The 'game changing' results from the RELATIVITY-047 trial validated LAG-3 blockade as a relevant biological target and established it as the third clinically relevant immune checkpoint. Importantly, LAG-3 inhibition in combination with PD-1 inhibition offered impressive efficacy with modest increases in toxicity over single agent PD-1 inhibitor and has been U.S. Food and Drug Administration approved for the first-line therapy of patients with metastatic melanoma. The efficacy of this combination in patients with untreated brain or leptomeningeal metastases or with rare melanoma types, such as uveal melanoma, remains to be established. The challenge remains to elucidate specific mechanisms of response and resistance to LAG-3 blockade and to extend its benefits to other malignancies. Ongoing trials are studying the combination of LAG-3 antibodies with PD-1 inhibitors in multiple cancers and settings. The low toxicity of the combination may also allow for further layering of additional therapeutic approaches such as chemotherapy, oncolytic viruses, cellular therapies, and possibly novel cytokines, among others.
尽管在过去十年中免疫疗法和靶向疗法取得了重大进展,但转移性黑色素瘤对近一半的患者来说仍然是一种致命疾病。在过去十年中,免疫谱分析的进展以及对免疫肿瘤微环境(TME)的更深入理解,使得针对黑色素瘤免疫疗法的新方法得以开发,并且有大量靶点正在研究中。然而,迄今为止,免疫检查点阻断仍然是最成功的方法,程序性细胞死亡蛋白1(PD-1)/程序性细胞死亡配体1(PD-L1)和细胞毒性T淋巴细胞相关抗原4(CTLA-4)抑制剂单独或联合使用,在转移性黑色素瘤患者中产生了最强劲和持久的临床疗效。PD-1和CTLA-4联合抑制实现了最高的持久缓解率,并且在包括脑转移在内的各种情况下都有效;然而,这是以高达60%的患者出现多种危及生命的毒性为代价的。这也使黑色素瘤成为免疫肿瘤学(IO)药物开发的前沿领域,并且一直在寻找新的检查点,包括T细胞免疫球蛋白和粘蛋白结构域包含3(TIM-3)、淋巴细胞激活基因3(LAG-3)、V结构域免疫球蛋白抑制T细胞激活(VISTA)、T细胞免疫球蛋白和基于免疫受体酪氨酸的抑制基序(ITIM)结构域(TIGIT)等多个相关靶点。淋巴细胞激活基因3(LAG-3)是T细胞上的一种共抑制受体,可抑制其激活,它彻底改变了黑色素瘤的免疫调节。RELATIVITY-047试验的“改变游戏规则”的结果证实LAG-3阻断是一个相关的生物学靶点,并将其确立为第三个临床相关的免疫检查点。重要的是,LAG-3抑制与PD-1抑制联合使用具有令人印象深刻的疗效,与单药PD-1抑制剂相比毒性略有增加,并且已获得美国食品药品监督管理局批准用于转移性黑色素瘤患者的一线治疗。这种联合疗法在未经治疗的脑或软脑膜转移患者或葡萄膜黑色素瘤等罕见黑色素瘤类型患者中的疗效仍有待确定。挑战仍然是阐明对LAG-3阻断的反应和耐药的具体机制,并将其益处扩展到其他恶性肿瘤。正在进行的试验正在研究LAG-3抗体与PD-1抑制剂在多种癌症和情况下的联合使用。这种联合疗法的低毒性也可能允许进一步叠加其他治疗方法,如化疗、溶瘤病毒、细胞疗法以及可能的新型细胞因子等。