Dayer Nicolas, Ltaief Zied, Liaudet Lucas, Lechartier Benoit, Aubert John-David, Yerly Patrick
Department of Cardiology, Lausanne University Hospital and Lausanne University, 1011 Lausanne, Switzerland.
Department of Adult Intensive Care Medicine, Lausanne University Hospital and Lausanne University, 1011 Lausanne, Switzerland.
J Clin Med. 2023 Jul 17;12(14):4722. doi: 10.3390/jcm12144722.
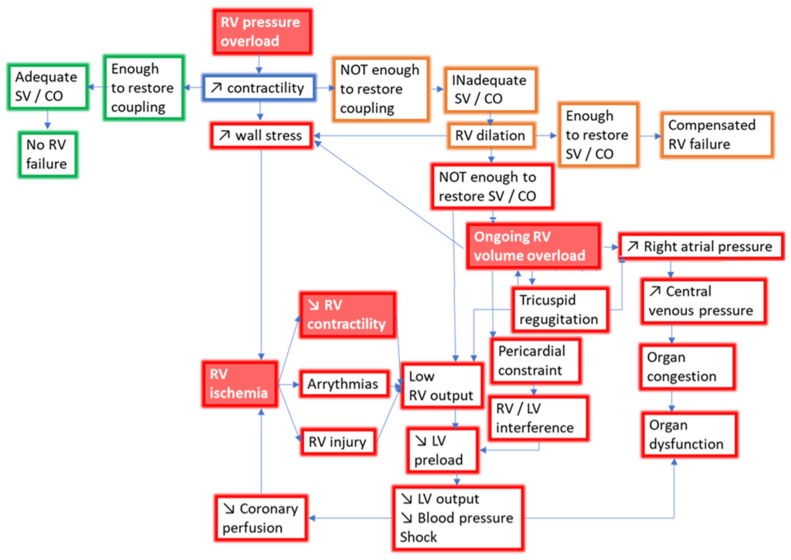
Right ventricular failure (RVF) is often caused by increased afterload and disrupted coupling between the right ventricle (RV) and the pulmonary arteries (PAs). After a phase of adaptive hypertrophy, pressure-overloaded RVs evolve towards maladaptive hypertrophy and finally ventricular dilatation, with reduced stroke volume and systemic congestion. In this article, we review the concept of RV-PA coupling, which depicts the interaction between RV contractility and afterload, as well as the invasive and non-invasive techniques for its assessment. The current principles of RVF management based on pathophysiology and underlying etiology are subsequently discussed. Treatment strategies remain a challenge and range from fluid management and afterload reduction in moderate RVF to vasopressor therapy, inotropic support and, occasionally, mechanical circulatory support in severe RVF.
右心室衰竭(RVF)通常由后负荷增加以及右心室(RV)与肺动脉(PA)之间的耦合破坏引起。在经历适应性肥厚阶段后,压力超负荷的右心室会发展为失适应性肥厚,最终导致心室扩张,每搏输出量减少并出现体循环淤血。在本文中,我们回顾了右心室-肺动脉耦合的概念,该概念描述了右心室收缩力与后负荷之间的相互作用,以及评估它的有创和无创技术。随后讨论了基于病理生理学和潜在病因的右心室衰竭管理的当前原则。治疗策略仍然是一项挑战,范围从中度右心室衰竭时的液体管理和后负荷降低到严重右心室衰竭时的血管升压药治疗、正性肌力支持以及偶尔的机械循环支持。