Stieb David M, Smith-Doiron Marc, Quick Matthew, Christidis Tanya, Xi Guoliang, Miles Rosalin M, van Donkelaar Aaron, Martin Randall V, Hystad Perry, Tjepkema Michael
Environmental Health Science and Research Bureau Health Canada Vancouver BC Canada.
Environmental Health Science and Research Bureau Health Canada Ottawa ON Canada.
Geohealth. 2023 Aug 29;7(9):e2023GH000816. doi: 10.1029/2023GH000816. eCollection 2023 Sep.
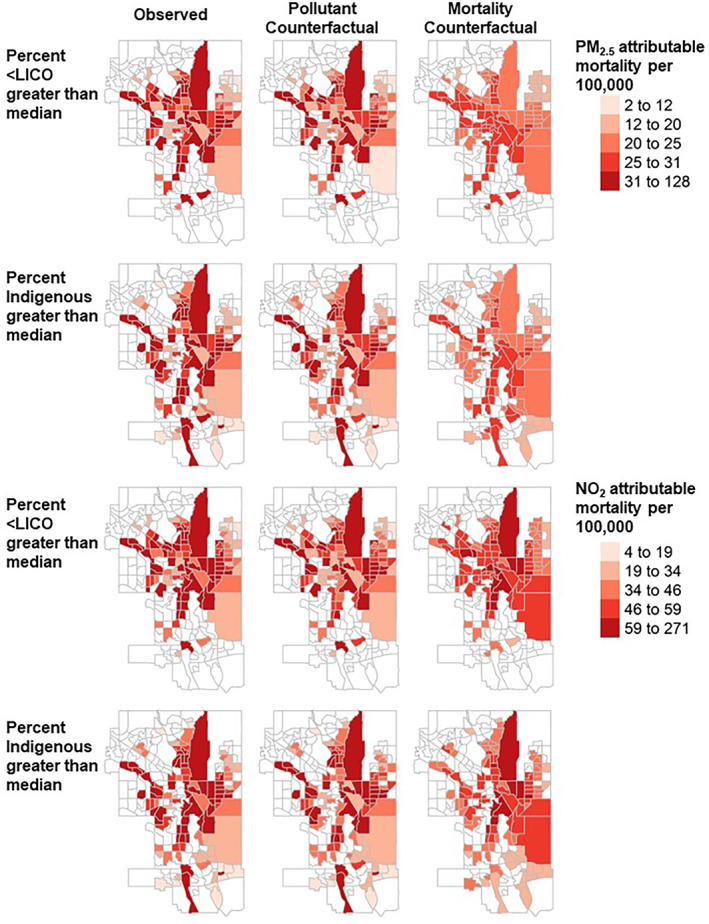
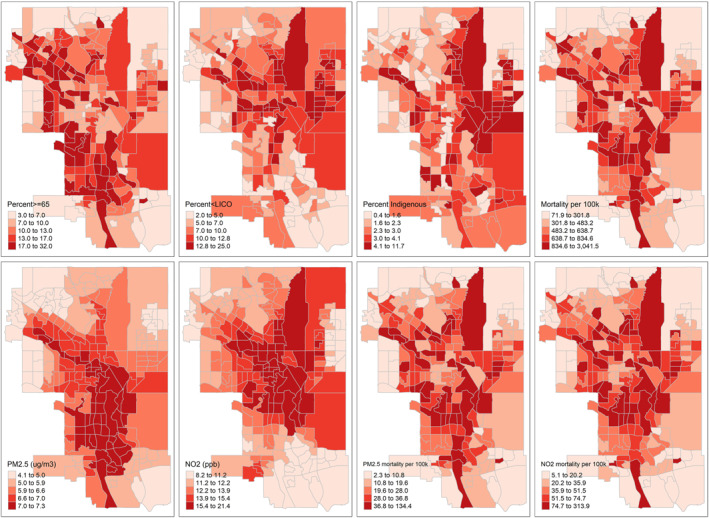
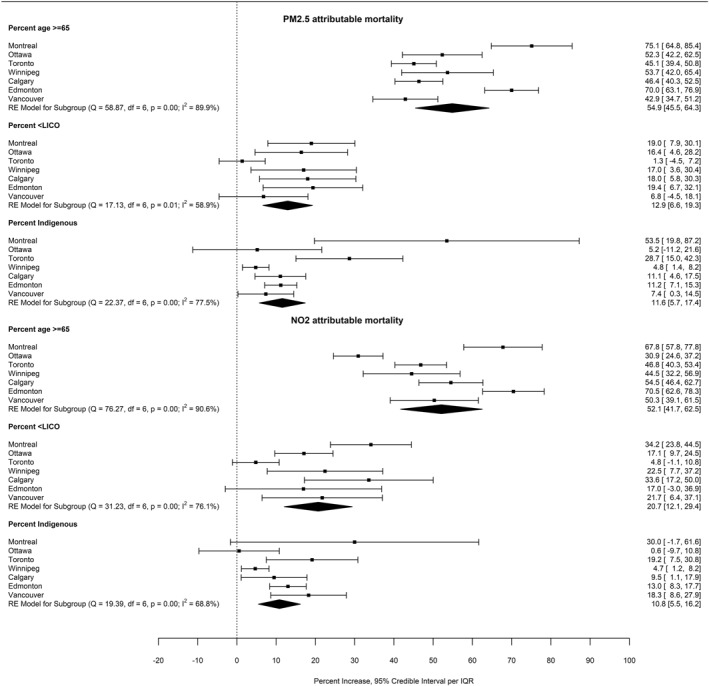
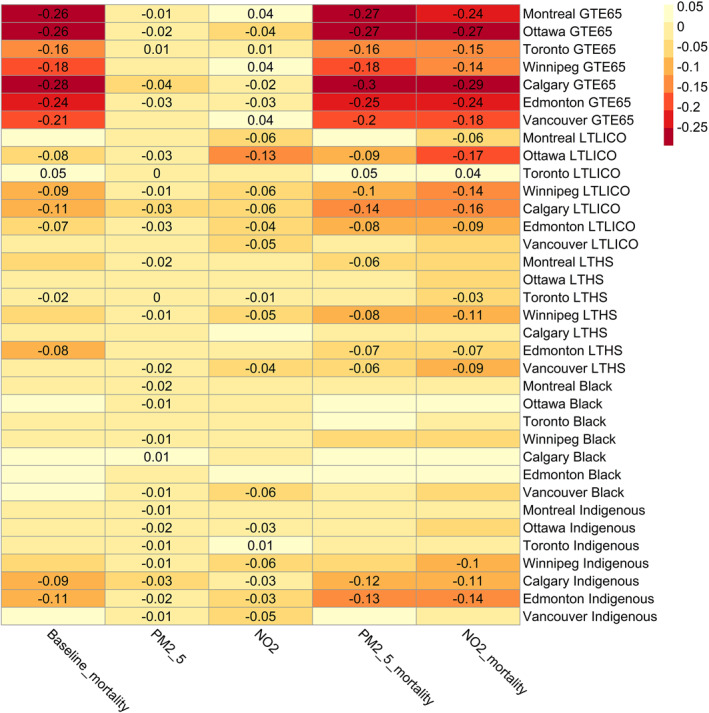
Recent studies have identified inequality in the distribution of air pollution attributable health impacts, but to our knowledge this has not been examined in Canadian cities. We evaluated the extent and sources of inequality in air pollution attributable mortality at the census tract (CT) level in seven of Canada's largest cities. We first regressed fine particulate matter (PM) and nitrogen dioxide (NO) attributable mortality against the neighborhood (CT) level prevalence of age 65 and older, low income, low educational attainment, and identification as an Indigenous (First Nations, Métis, Inuit) or Black person, accounting for spatial autocorrelation. We next examined the distribution of baseline mortality rates, PM and NO concentrations, and attributable mortality by neighborhood (CT) level prevalence of these characteristics, calculating the concentration index, Atkinson index, and Gini coefficient. Finally, we conducted a counterfactual analysis of the impact of reducing baseline mortality rates and air pollution concentrations on inequality in air pollution attributable mortality. Regression results indicated that CTs with a higher prevalence of low income and Indigenous identity had significantly higher air pollution attributable mortality. Concentration index, Atkinson index, and Gini coefficient values revealed different degrees of inequality among the cities. Counterfactual analysis indicated that inequality in air pollution attributable mortality tended to be driven more by baseline mortality inequalities than exposure inequalities. Reducing inequality in air pollution attributable mortality requires reducing disparities in both baseline mortality and air pollution exposure.
近期研究已确定空气污染所致健康影响的分布存在不平等现象,但据我们所知,加拿大各城市尚未对此进行过研究。我们评估了加拿大七个最大城市中人口普查区(CT)层面空气污染所致死亡率不平等的程度和来源。我们首先将细颗粒物(PM)和二氧化氮(NO)所致死亡率与65岁及以上、低收入、低教育程度以及被认定为原住民(第一民族、梅蒂斯、因纽特)或黑人的社区(CT)层面患病率进行回归分析,同时考虑空间自相关性。接下来,我们按这些特征的社区(CT)层面患病率,研究了基线死亡率、PM和NO浓度以及所致死亡率的分布情况,计算了浓度指数、阿特金森指数和基尼系数。最后,我们对降低基线死亡率和空气污染浓度对空气污染所致死亡率不平等的影响进行了反事实分析。回归结果表明,低收入和原住民身份患病率较高的人口普查区空气污染所致死亡率显著更高。浓度指数、阿特金森指数和基尼系数值揭示了各城市不同程度的不平等现象。反事实分析表明,空气污染所致死亡率的不平等往往更多地由基线死亡率不平等而非暴露不平等所驱动。减少空气污染所致死亡率的不平等需要减少基线死亡率和空气污染暴露方面的差距。