Alizada Merve, Sahin Turgut, Sener Ozden, Kocyigit Pelin
Department of Dermatology, Mamak State Hospital, 06230 Ankara, Turkey.
Department of Neurology, Cankırı State Hospital, 18100 Çankırı, Turkey.
Diagnostics (Basel). 2023 Dec 22;14(1):23. doi: 10.3390/diagnostics14010023.
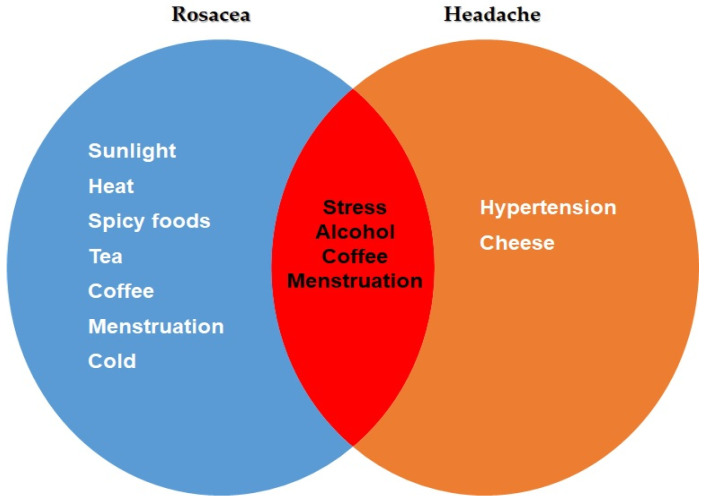
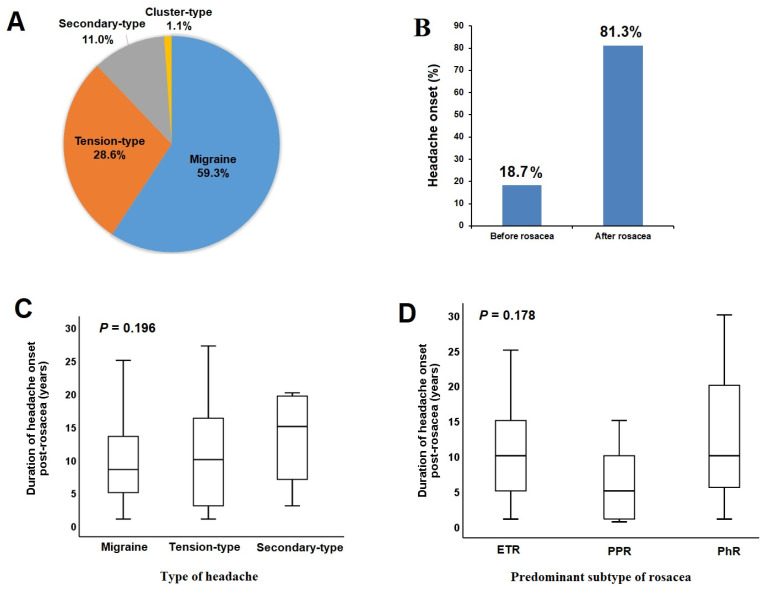
This study aimed to investigate the relationship between rosacea and headaches, focusing on different subtypes, as well as the associated clinical features and triggering factors. In this prospective study, 300 patients diagnosed with rosacea and 320 control subjects without rosacea or any connected mast cell activation illness were included. Patients with rosacea were assessed by a dermatologist according to the 2019 updated rosacea classification (ROSCO panel). Accordingly, patients were classified based on their predominant rosacea subtype as follows: erythematotelangiectatic (ETR), papulopustular (PPR), or phymatous (RhR). Patients experiencing headaches were assessed using the International Headache Classification. Headaches were categorized as migraine, tension-type headaches (TTHs), secondary types (STHs), and cluster-type headaches (CTHs). The ratio of headache was 30.3% in the rosacea group, which did not show a significant difference compared to the control group (30.3% vs. 25.0%, = 0.138). In 81.3% of rosacea patients with headaches, headache onset occurred after the diagnosis of rosacea. The rate of patients with headaches was higher in the ETR group compared to the PPR and RhR groups (35.2% vs. 16.2% vs. 23.1%, = 0.007, respectively). In terms of headache subtypes, the rates of patients with migraine and STHs were higher in the ETR group compared to the PPR and RhR groups, while the rate of patients with TTHs was higher in the RhR group. A positive correlation was found between rosacea severity and migraine severity (r = 0.284, < 0.05). Among the triggering factors for rosacea, only sunlight was found to be associated with headaches. Lower age, female gender, and moderate to severe rosacea severity were identified as independent factors increasing the likelihood of headaches. A significant portion of rosacea patients experience headaches. Particularly, different subtypes of rosacea may be associated with various types of headaches. This study, highlighting the connection between migraine and ETR, is a pioneering work that demonstrates common pathogenic mechanisms and potential triggers.
本研究旨在调查酒渣鼻与头痛之间的关系,重点关注不同亚型以及相关的临床特征和诱发因素。在这项前瞻性研究中,纳入了300例被诊断为酒渣鼻的患者和320例无酒渣鼻或任何相关肥大细胞活化疾病的对照受试者。酒渣鼻患者由皮肤科医生根据2019年更新的酒渣鼻分类(ROSCO小组)进行评估。据此,患者根据其主要的酒渣鼻亚型分类如下:红斑毛细血管扩张型(ETR)、丘疹脓疱型(PPR)或鼻赘型(RhR)。经历头痛的患者使用国际头痛分类进行评估。头痛分为偏头痛、紧张型头痛(TTH)、继发性头痛(STH)和丛集性头痛(CTH)。酒渣鼻组的头痛发生率为30.3%,与对照组相比无显著差异(30.3%对25.0%,P = 0.138)。在81.3%的有头痛的酒渣鼻患者中,头痛发作发生在酒渣鼻诊断之后。ETR组头痛患者的比例高于PPR组和RhR组(分别为35.2%对16.2%对23.1%,P = 0.007)。在头痛亚型方面,ETR组偏头痛和STH患者的比例高于PPR组和RhR组,而RhR组TTH患者的比例更高。发现酒渣鼻严重程度与偏头痛严重程度之间存在正相关(r = 0.284,P < 0.05)。在酒渣鼻的诱发因素中,仅发现阳光与头痛有关。年龄较小、女性性别以及中度至重度酒渣鼻严重程度被确定为增加头痛可能性的独立因素。相当一部分酒渣鼻患者会经历头痛。特别是,不同亚型的酒渣鼻可能与各种类型的头痛有关。这项突出偏头痛与ETR之间联系的研究是一项开创性工作,证明了共同的致病机制和潜在触发因素。