Jia Xiu-Fen, Chen Yong-Chun, Zheng Kui-Kui, Zhu Dong-Qin, Chen Chao, Liu Jinjin, Yang Yun-Jun, Li Chuan-Ting
Department of Radiology, Shandong Provincial Hospital, Shandong University, Jinan, 250021, People's Republic of China.
Department of Radiology, First Affiliated Hospital of Wenzhou Medical University, Wenzhou, 325000, People's Republic of China.
J Multidiscip Healthc. 2024 Dec 10;17:5917-5926. doi: 10.2147/JMDH.S491697. eCollection 2024.
Risk estimation of intracranial aneurysm rupture is critical in determining treatment strategy. There is a scarcity of multicenter studies on the predictive power of clinical-radiomics models for aneurysm rupture. This study aims to develop a clinical-radiomics model and explore its additional value in the discrimination of aneurysm rupture.
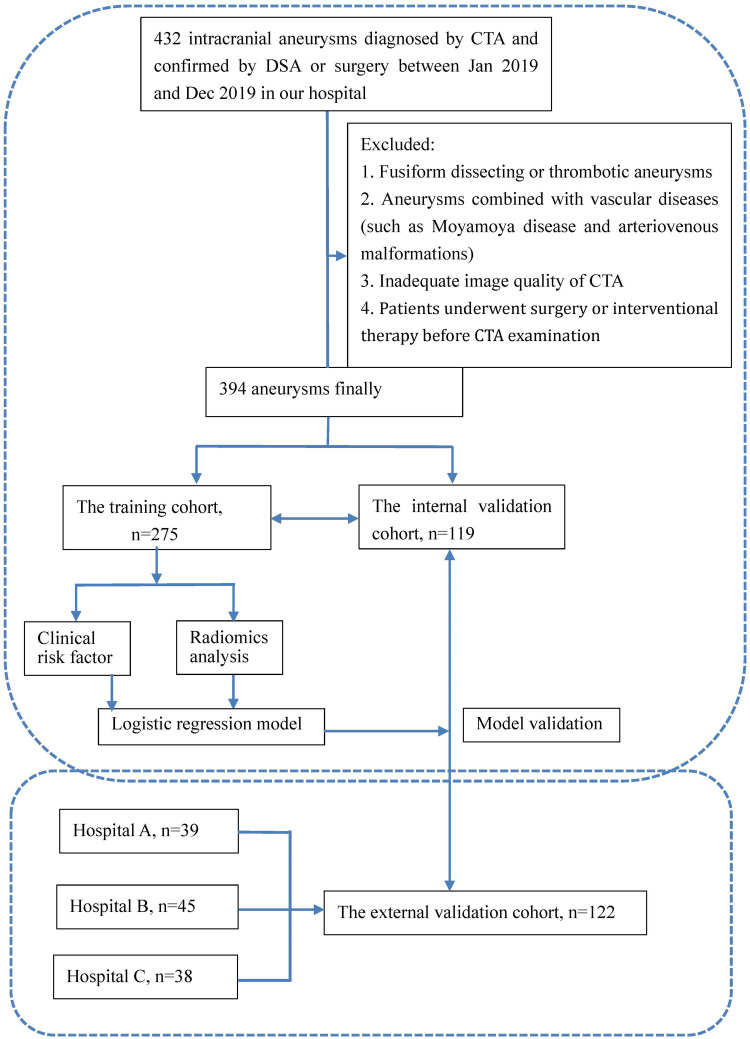
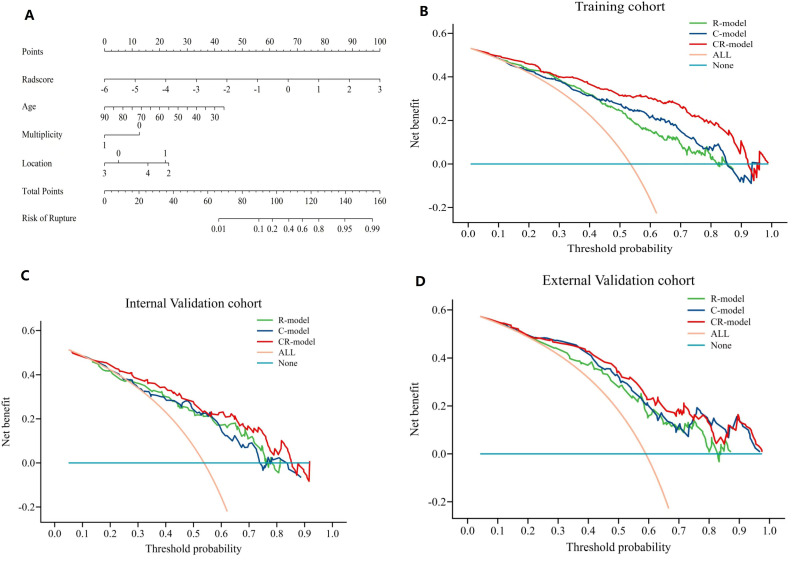
A total of 516 aneurysms, including 273 (52.9%) with ruptured aneurysms, were retrospectively enrolled from four hospitals between January 2019 and August 2020. Relevant clinical features were collected, and radiomic characteristics associated with aneurysm were extracted. Subsequently, three models, including a clinical model, a radiomics model, and a clinical-radiomics model were constructed using multivariate logistic regression analysis to effectively classify aneurysm rupture. The performance of models was analyzed through operating characteristic curves, decision curve, and calibration curves analysis. Different models' comparison used DeLong tests. To offer an understandable and intuitive scoring system for assessing rupture risk, we developed a comprehensive nomogram based on the developed model.
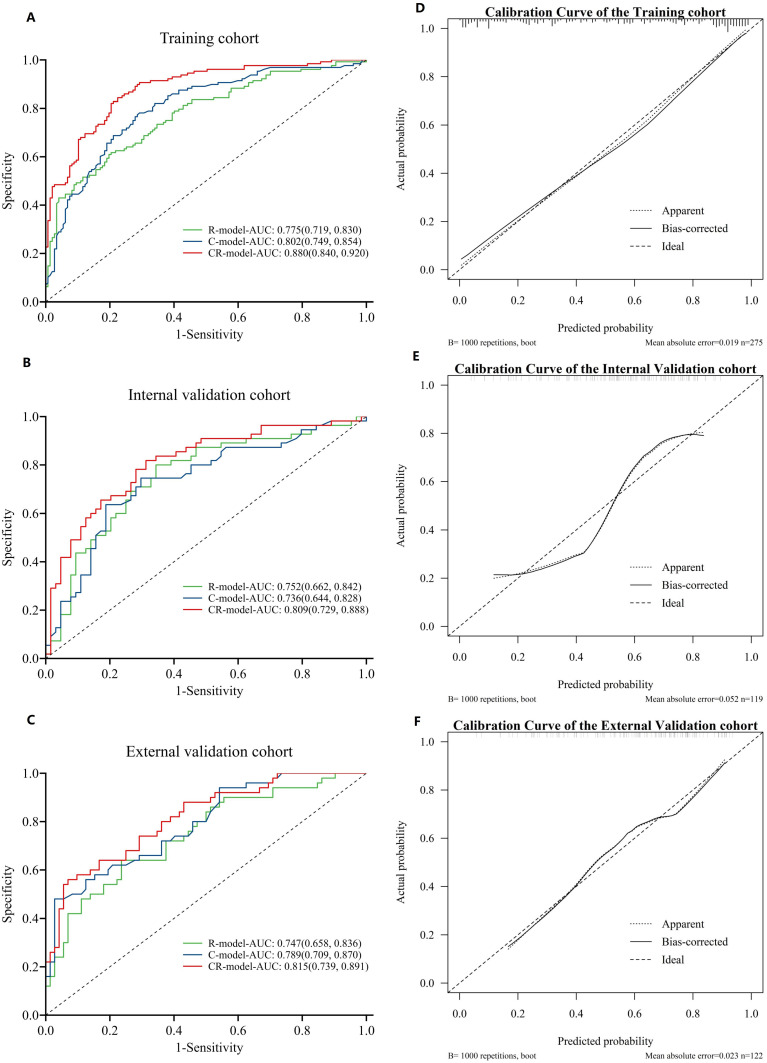
Three clinical risk factors and fourteen radiomics features were explored to establish three models. The area under the receiver operating curve (AUC) for the radiomics model was 0.775 (95% CI,0.719-0.830), 0.752 (95% CI,0.663-0.841), 0.747 (95% CI,0.658-0.835) in the training, internal and external test datasets, respectively. The AUC for clinical model was 0.802 (95% CI, 0.749-0.854), 0.736 (95% CI, 0.644-0.828), 0.789 (95% CI, 0.709-0.870) in these three sets, respectively. The clinical-radiomics model showed an AUC of 0.880 (95% CI,0.840-0.920), 0.807 (95% CI,0.728-0.887), 0.815 (95% CI,0.740-0.891) in three datasets respectively. Compared with the radiomics and clinical models, the clinical-radiomics model demonstrated better diagnostic performance (DeLong' test P < 0.05).
The clinical-radiomics model represents a promising approach for predicting rupture of intracranial aneurysms.
颅内动脉瘤破裂风险评估对于确定治疗策略至关重要。关于临床-放射组学模型对动脉瘤破裂预测能力的多中心研究较少。本研究旨在建立一种临床-放射组学模型,并探讨其在鉴别动脉瘤破裂方面的附加价值。
回顾性纳入2019年1月至2020年8月期间四家医院的516个动脉瘤,其中273个(52.9%)为破裂动脉瘤。收集相关临床特征,并提取与动脉瘤相关的放射组学特征。随后,采用多因素逻辑回归分析构建临床模型、放射组学模型和临床-放射组学模型,以有效区分动脉瘤破裂情况。通过操作特征曲线、决策曲线和校准曲线分析来评估模型性能。不同模型的比较采用DeLong检验。为提供一个易于理解和直观的评分系统来评估破裂风险,我们基于所建立的模型开发了一个综合列线图。
探索了三个临床风险因素和14个放射组学特征来建立三个模型。放射组学模型在训练集、内部测试集和外部测试集中的受试者操作曲线下面积(AUC)分别为0.775(95%CI,0.719-0.830)、0.752(95%CI,0.663-0.841)、0.747(95%CI,0.658-0.835)。临床模型在这三个数据集中的AUC分别为0.802(95%CI,0.749-0.854)、0.736(95%CI,0.644-0.828)、0.789(95%CI,0.709-0.870)。临床-放射组学模型在三个数据集中的AUC分别为0.880(95%CI,0.840-0.920)、0.807(95%CI,0.728-0.887)、0.815(95%CI,0.740-0.891)。与放射组学模型和临床模型相比,临床-放射组学模型表现出更好的诊断性能(DeLong检验P<0.05)。
临床-放射组学模型是预测颅内动脉瘤破裂的一种有前景的方法。