Friedman A H
Trans Am Ophthalmol Soc. 1984;82:447-91.
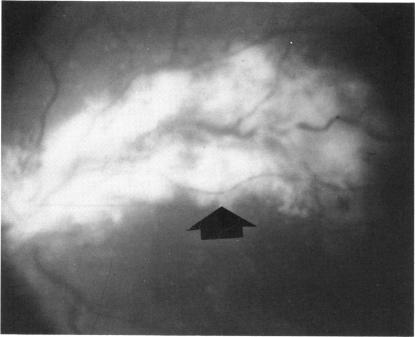
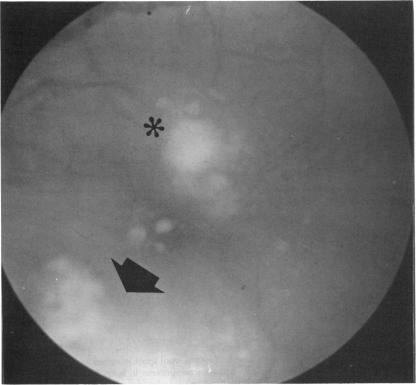
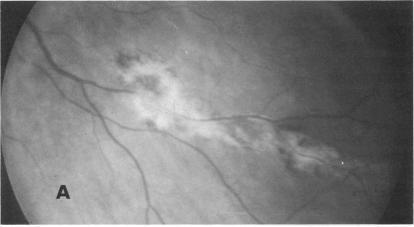
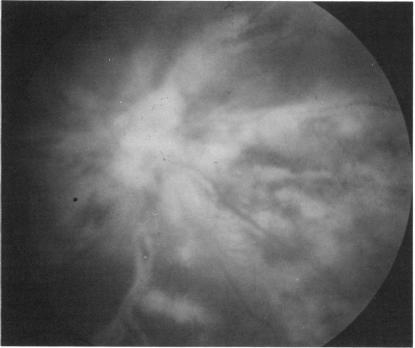
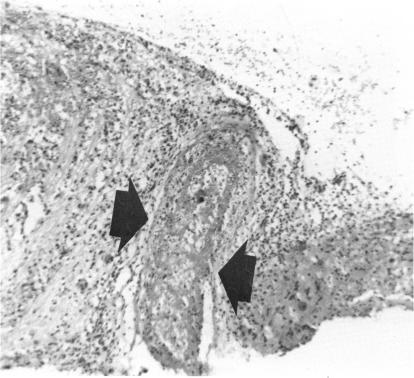
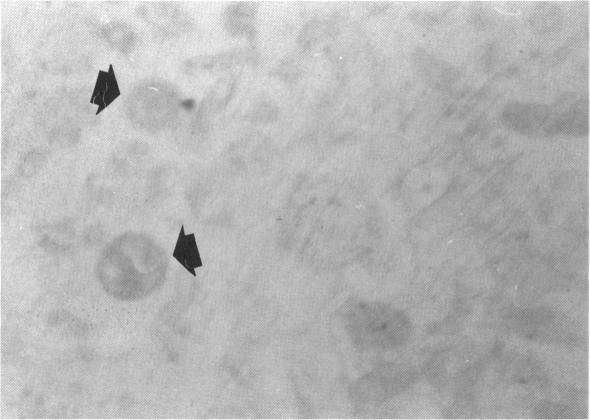
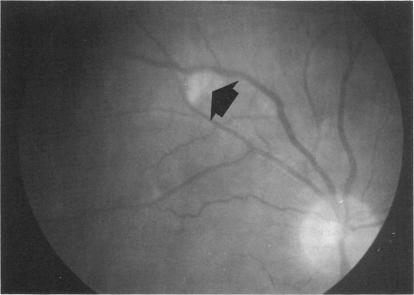
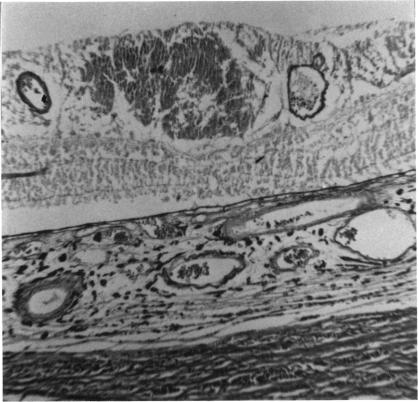
AIDS is a reliably diagnosed disease that is indicative of an underlying cellular immunodeficiency with no other cause for the disorder. To date over 2000 cases have been reported in North America and Europe and the number is rising. Patients fulfilling the definition for AIDS have included male homosexuals, IV drug abusers of both sexes, people from Haiti, heterosexual partners of AIDS patients, hemophiliacs, and some patients who fit no particular pattern. The etiology has been attributed to factors acting singly or in synergy namely that repeated exposure to CMV, semen, or other antigens results in progressive cellular immunodeficiency, or alternatively, a novel virus has an etiologic role. The epidemiology of the syndrome suggests a horizontally transmissible agent. The spectrum of opportunistic infections observed in AIDS patients is well documented. A higher incidence of KS as well as squamous carcinoma of the oral cavity, cloacogenic carcinoma of the rectum, primary lymphomas of the brain, and systemic Burkitt's-like lymphoma has been noted. Seventy-one patients with AIDS were examined and followed during the course of their disease. Forty-one patients had definite retinal lesions at the time of examination. The most common intraretinal finding was CMV retinitis which displayed the typical white, crumbly areas of retinal necrosis and hemorrhage. Optic nerve involvement was quite common. The development of retinitis was a harbinger of eventual death as it was a progressive and a nontreatable disorder, lasting about 6 months. The second most common retinal finding was cotton wool spots, the lesions were usually present during the course of PCP and were due to microvascular damage in the retina from circulating immune complexes. No organisms were demonstrated in the retina. One AIDS patient who had been an IV drug abuser developed fungal retinitis due to Candida albicans. The patient eventually died from Candida sepsis. One patient had acquired toxoplasmosis retinochoroiditis. Examination revealed a large active intraretinal focus of infection. No other retinal lesion was noted. The patient, a homosexual, died from a toxoplasmosis brain abscess. The patient with AIDS is in a continuing struggle for survival against a myriad assortment of opportunistic infectious agents. Careful initial ophthalmological examination and long-term follow-up are mandatory.
艾滋病是一种诊断明确的疾病,它表明存在潜在的细胞免疫缺陷且无其他病因。迄今为止,北美和欧洲已报告了2000多例病例,且数量还在上升。符合艾滋病定义的患者包括男性同性恋者、男女静脉注射吸毒者、海地人、艾滋病患者的异性伴侣、血友病患者以及一些无特定模式的患者。病因被归因于单独或协同起作用的因素,即反复接触巨细胞病毒、精液或其他抗原会导致进行性细胞免疫缺陷,或者一种新型病毒具有病因学作用。该综合征的流行病学表明存在一种水平传播的病原体。艾滋病患者中观察到的机会性感染范围有充分记录。已注意到卡波西肉瘤以及口腔鳞状癌、直肠泄殖腔癌、原发性脑淋巴瘤和系统性伯基特样淋巴瘤的发病率较高。对71例艾滋病患者在疾病过程中进行了检查和随访。41例患者在检查时有明确的视网膜病变。视网膜内最常见的发现是巨细胞病毒性视网膜炎,其表现为典型的白色、易碎的视网膜坏死和出血区域。视神经受累相当常见。视网膜炎的发展是最终死亡的先兆,因为它是一种进行性且无法治疗的疾病,持续约6个月。第二常见的视网膜发现是棉絮斑,这些病变通常在卡氏肺孢子虫肺炎病程中出现,是由循环免疫复合物导致的视网膜微血管损伤引起的。视网膜中未发现病原体。一名曾是静脉注射吸毒者的艾滋病患者因白色念珠菌感染发展为真菌性视网膜炎。该患者最终死于念珠菌败血症。一名患者患了弓形虫性视网膜脉络膜炎。检查发现视网膜内有一个大的活动性感染灶。未发现其他视网膜病变。该患者是一名同性恋者,死于弓形虫性脑脓肿。艾滋病患者正在与各种各样的机会性感染病原体进行持续的生存斗争。必须进行仔细的初始眼科检查和长期随访。