Mordon Serge R, Wassmer Benjamin, Zemmouri Jaouad
INSERM (French National Institute of Health and Medical Research) IFR 114, Lille University Hospital, Lille, France.
Biomed Eng Online. 2006 Apr 25;5:26. doi: 10.1186/1475-925X-5-26.
Endovenous laser treatment (ELT) has been recently proposed as an alternative in the treatment of reflux of the Great Saphenous Vein (GSV) and Small Saphenous Vein (SSV). Successful ELT depends on the selection of optimal parameters required to achieve an optimal vein damage while avoiding side effects. Mathematical modeling of ELT could provide a better understanding of the ELT process and could determine the optimal dosage as a function of vein diameter.
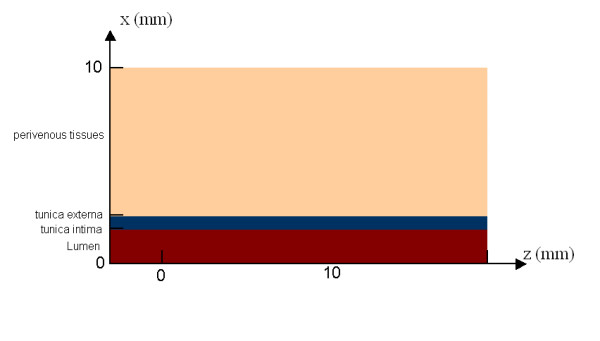
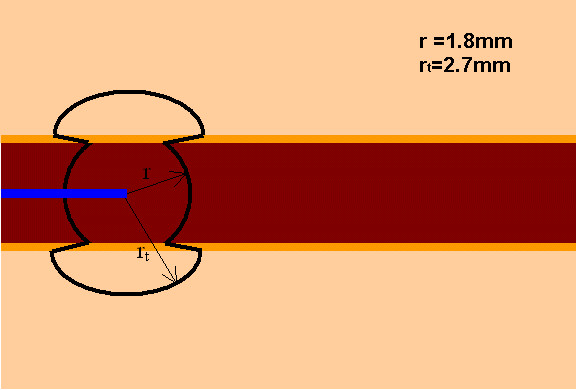
STUDY DESIGN/MATERIALS AND METHODS: The model is based on calculations describing the light distribution using the diffusion approximation of the transport theory, the temperature rise using the bioheat equation and the laser-induced injury using the Arrhenius damage model. The geometry to simulate ELT was based on a 2D model consisting of a cylindrically symmetric blood vessel including a vessel wall and surrounded by an infinite homogenous tissue. The mathematical model was implemented using the Macsyma-Pdease2D software (Macsyma Inc., Arlington, MA, USA). Damage to the vein wall for CW and single shot energy was calculated for 3 and 5 mm vein diameters. In pulsed mode, the pullback distance (3, 5 and 7 mm) was considered. For CW mode simulation, the pullback speed (1, 2, 3 mm/s) was the variable. The total dose was expressed as joules per centimeter in order to perform comparison to results already reported in clinical studies.
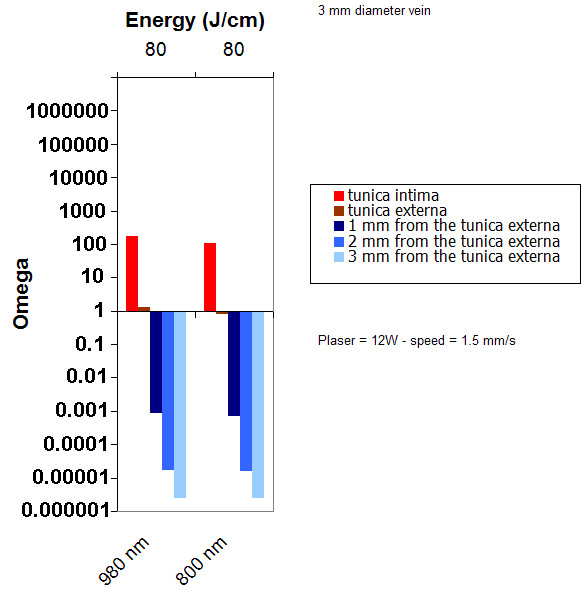
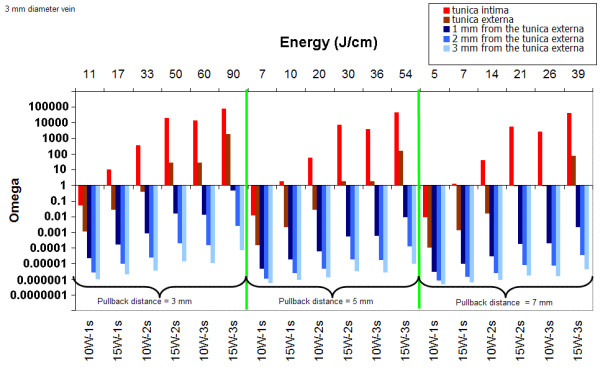
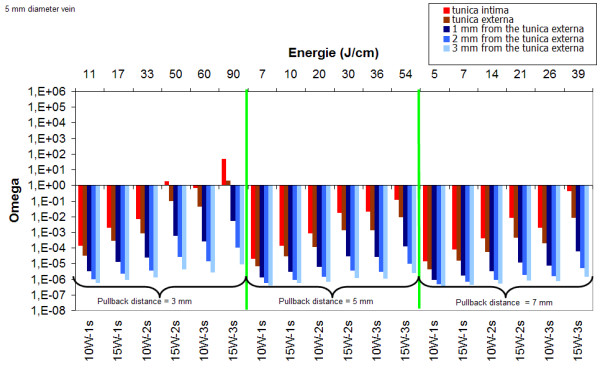
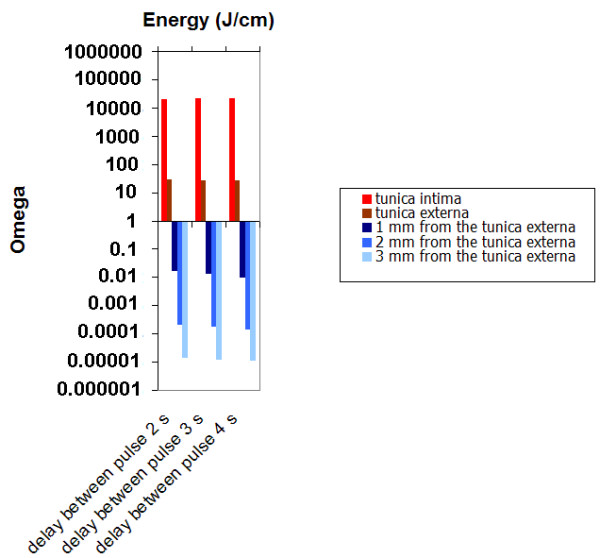
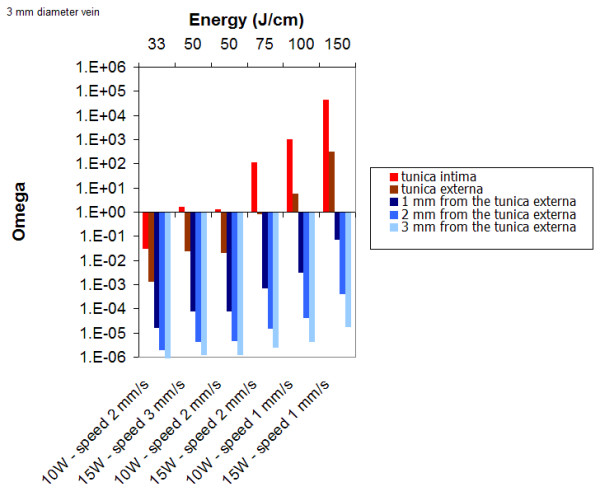
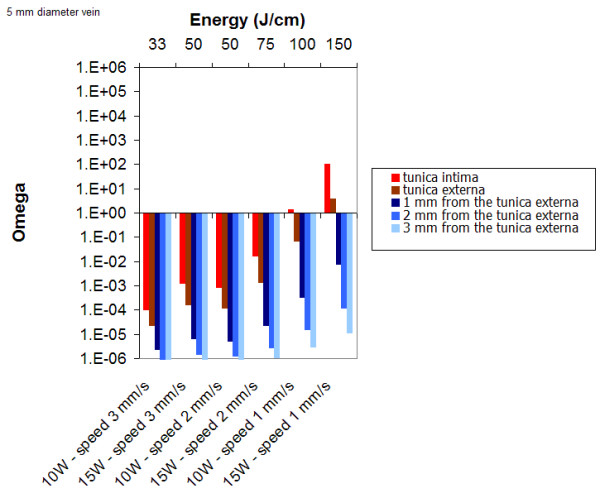
In pulsed mode, for a 3 mm vein diameter, irrespective of the pullback distance (2, 5 or 7 mm), a minimum fluence of 15 J/cm is required to obtain a permanent damage of the intima. For a 5 mm vein diameter, 50 J/cm (15W-2s) is required. In continuous mode, for a 3 mm and 5 mm vein diameter, respectively 65 J/cm and 100 J/cm are required to obtain a permanent damage of the vessel wall. Finally, the use of different wavelengths (810 nm or 980 nm) played only a minor influence on these results.
The parameters determined by mathematical modeling are in agreement with those used in clinical practice. They confirm that thermal damage of the inner vein wall (tunica intima) is required to achieve the tissue alterations necessary in order to lead the vein to permanent occlusion. However, in order to obtain a high rate of success without adverse events, the knowledge of the vein diameter after tumescent anesthesia is recommended in order to use the optimal energy. As clearly demonstrated by our calculations, both pulsed and continuous mode operations of the laser can be efficient. An interesting observation in our model is that less amount of energy is required in pulsed mode than in continuous mode. Damaging the vein sequentially along its entire length may lead to permanent occlusion. However, the pulsed mode requires a very precise positioning of the fiber after each pullback and the duration of the treatment is much longer. For these reasons, continuous irradiation seems to be preferred by most clinicians. This model should serve as a useful tool to simulate and better understand the mechanism of action of the ELT.

最近,静脉腔内激光治疗(ELT)已被提议作为治疗大隐静脉(GSV)和小隐静脉(SSV)反流的一种替代方法。成功的ELT取决于选择最佳参数,以实现最佳的静脉损伤,同时避免副作用。ELT的数学模型可以更好地理解ELT过程,并可以根据静脉直径确定最佳剂量。
研究设计/材料与方法:该模型基于使用输运理论的扩散近似描述光分布、使用生物热方程描述温度升高以及使用阿伦尼乌斯损伤模型描述激光诱导损伤的计算。模拟ELT的几何形状基于一个二维模型,该模型由一个包括血管壁并被无限均匀组织包围的圆柱对称血管组成。数学模型使用Macsyma-Pdease2D软件(美国马萨诸塞州阿灵顿的Macsyma公司)实现。计算了3毫米和5毫米静脉直径下连续波(CW)和单次能量对静脉壁的损伤。在脉冲模式下,考虑了回撤距离(3、5和7毫米)。对于连续波模式模拟,回撤速度(1、2、3毫米/秒)是变量。总剂量以焦耳每厘米表示,以便与临床研究中已报道的结果进行比较。
在脉冲模式下,对于3毫米的静脉直径,无论回撤距离(2、5或7毫米)如何,内膜永久性损伤所需的最小能量密度为15焦/厘米。对于5毫米的静脉直径,需要能量密度50焦/厘米(15瓦-2秒)。在连续模式下,对于3毫米和5毫米的静脉直径,分别需要65焦/厘米和100焦/厘米才能使血管壁产生永久性损伤。最后,使用不同波长(810纳米或980纳米)对这些结果的影响很小。
数学建模确定的参数与临床实践中使用的参数一致。它们证实,为了使静脉永久性闭塞,需要对静脉内壁(内膜)进行热损伤,以实现必要的组织改变。然而,为了在无不良事件的情况下获得高成功率,建议了解肿胀麻醉后的静脉直径,以便使用最佳能量。正如我们的计算清楚表明的那样,激光的脉冲和连续模式操作都可以有效。我们模型中的一个有趣观察结果是,脉冲模式比连续模式所需的能量更少。沿着静脉的整个长度依次损伤静脉可能导致永久性闭塞。然而,脉冲模式需要在每次回撤后非常精确地定位光纤,并且治疗持续时间要长得多。由于这些原因,大多数临床医生似乎更喜欢连续照射。该模型应作为一个有用的工具,用于模拟和更好地理解ELT的作用机制。