Unlü Cağdaş, de Korte Niels, Daniels Lidewine, Consten Esther C J, Cuesta Miguel A, Gerhards Michael F, van Geloven Anna A W, van der Zaag Edwin S, van der Hoeven Joost A B, Klicks Rutger, Cense Huib A, Roumen Rudi M H, Eijsbouts Quirijn A J, Lange Johan F, Fockens Paul, de Borgie Corianne A J M, Bemelman Wilem A, Reitsma Johannes B, Stockmann Hein B A C, Vrouenraets Bart C, Boermeester Marja A
Department of Surgery, Sint Lucas Andreas Hospital Amsterdam, the Netherlands.
BMC Surg. 2010 Jul 20;10:23. doi: 10.1186/1471-2482-10-23.
Conservative treatment of uncomplicated or mild diverticulitis usually includes antibiotic therapy. It is, however, uncertain whether patients with acute diverticulitis indeed benefit from antibiotics. In most guidelines issued by professional organizations antibiotics are considered mandatory in the treatment of mild diverticulitis. This advice lacks evidence and is merely based on experts' opinion. Adverse effects of the use of antibiotics are well known, including allergic reactions, development of bacterial resistance to antibiotics and other side-effects.
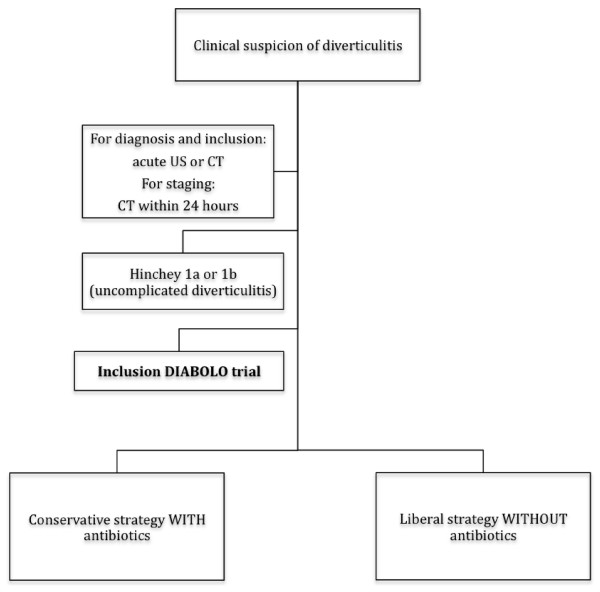
A randomized multicenter pragmatic clinical trial comparing two treatment strategies for uncomplicated acute diverticulitis. I) A conservative strategy with antibiotics: hospital admission, supportive measures and at least 48 hours of intravenous antibiotics which subsequently are switched to oral, if tolerated (for a total duration of antibiotic treatment of 10 days). II) A liberal strategy without antibiotics: admission only if needed on clinical grounds, supportive measures only. Patients are eligible for inclusion if they have a diagnosis of acute uncomplicated diverticulitis as demonstrated by radiological imaging. Only patients with stages 1a and 1b according to Hinchey's classification or "mild" diverticulitis according to the Ambrosetti criteria are included. The primary endpoint is time-to-full recovery within a 6-month follow-up period. Full recovery is defined as being discharged from the hospital, with a return to pre-illness activities, and VAS score below 4 without the use of daily pain medication. Secondary endpoints are proportion of patients who develop complicated diverticulitis requiring surgery or non-surgical intervention, morbidity, costs, health-related quality of life, readmission rate and acute diverticulitis recurrence rate. In a non-inferiority design 264 patients are needed in each study arm to detect a difference in time-to-full recovery of 5 days or more with a power of 85% and a confidence level of 95%. With an estimated one percent of patients lost to follow up, a total of 533 patients will be included.
A clinically relevant difference of more than 5 days in time-to-full recovery between the two treatment strategies is not expected. The liberal strategy without antibiotics and without the strict requirement for hospital admission is anticipated to be more a more cost-effective approach.
NCT01111253.
单纯性或轻度憩室炎的保守治疗通常包括抗生素治疗。然而,急性憩室炎患者是否真的能从抗生素治疗中获益尚不确定。在专业组织发布的大多数指南中,抗生素被认为是治疗轻度憩室炎的必需药物。这一建议缺乏证据,仅仅基于专家意见。使用抗生素的不良反应众所周知,包括过敏反应、细菌对抗生素产生耐药性以及其他副作用。
一项随机多中心实用临床试验,比较两种治疗单纯性急性憩室炎的策略。I)使用抗生素的保守策略:住院、支持性措施以及至少48小时的静脉抗生素治疗,若耐受则随后改为口服(抗生素治疗总时长为10天)。II)不使用抗生素的宽松策略:仅在临床需要时住院,仅采取支持性措施。如果患者经影像学检查确诊为急性单纯性憩室炎,则符合纳入标准。仅纳入根据辛奇分类法为1a期和1b期或根据安布罗塞蒂标准为“轻度”憩室炎的患者。主要终点是6个月随访期内完全康复的时间。完全康复定义为出院、恢复病前活动且视觉模拟评分(VAS)低于4分且无需每日使用止痛药物。次要终点包括发生需要手术或非手术干预的复杂性憩室炎的患者比例、发病率、费用、健康相关生活质量、再入院率和急性憩室炎复发率。在非劣效性设计中,每个研究组需要264例患者,以85%的检验效能和95%的置信水平检测完全康复时间的差异是否达到5天或更长。估计有1%的患者失访,总共将纳入533例患者。
预计两种治疗策略在完全康复时间上的临床相关差异不会超过5天。不使用抗生素且对住院没有严格要求的宽松策略预计将是一种更具成本效益的方法。
NCT01111253。