School of Computer Science and Software Engineering, University of Western Australia, Crawley, Australia.
PLoS One. 2010 Nov 3;5(11):e13797. doi: 10.1371/journal.pone.0013797.
Neuraminidase inhibitors were used to reduce the transmission of pandemic influenza A/H1N1 2009 at the early stages of the 2009/2010 pandemic. Policies for diagnosis of influenza for the purposes of antiviral intervention differed markedly between and within countries, leading to differences in the timing and scale of antiviral usage.
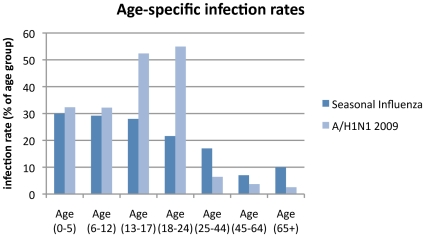
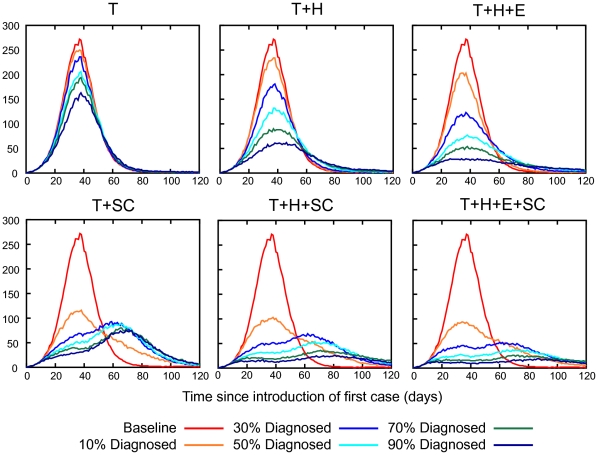
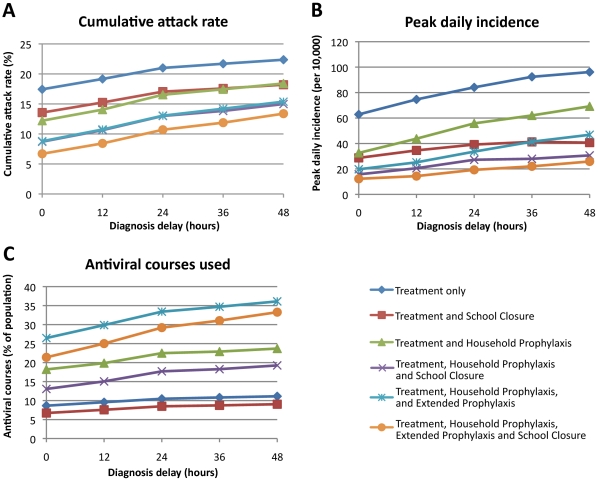
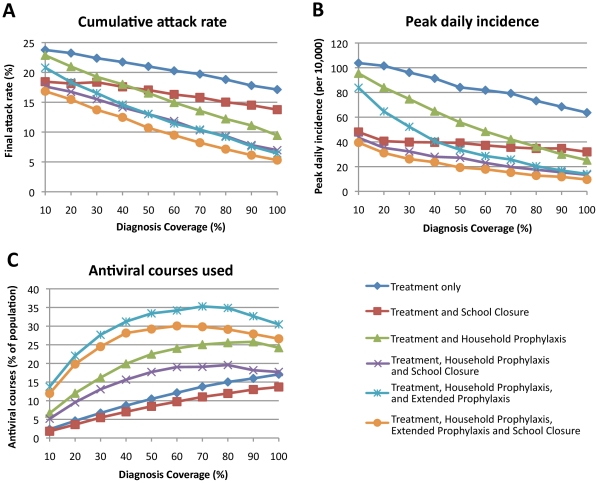
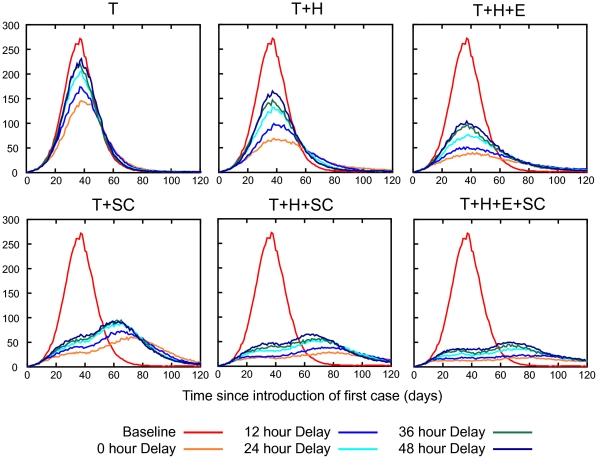
METHODOLOGY/PRINCIPAL FINDINGS: The impact of the percentage of symptomatic infected individuals who were diagnosed, and of delays to diagnosis, for three antiviral intervention strategies (each with and without school closure) were determined using a simulation model of an Australian community. Epidemic characteristics were based on actual data from the A/H1N1 2009 pandemic including reproduction number, serial interval and age-specific infection rate profile. In the absence of intervention an illness attack rate (AR) of 24.5% was determined from an estimated R(0) of 1.5; this was reduced to 21%, 16.5% or 13% by treatment-only, treatment plus household prophylaxis, or treatment plus household plus extended prophylaxis antiviral interventions respectively, assuming that diagnosis occurred 24 hours after symptoms arose and that 50% of symptomatic cases were diagnosed. If diagnosis occurred without delay, ARs decreased to 17%, 12.2% or 8.8% respectively. If 90% of symptomatic cases were diagnosed (with a 24 hour delay), ARs decreased to 17.8%, 11.1% and 7.6%, respectively.
The ability to rapidly diagnose symptomatic cases and to diagnose a high proportion of cases was shown to improve the effectiveness of all three antiviral strategies. For epidemics with R(0)< = 1.5 our results suggest that when the case diagnosis coverage exceeds ∼70% the size of the antiviral stockpile required to implement the extended prophylactic strategy decreases. The addition of at least four weeks of school closure was found to further reduce cumulative and peak attack rates and the size of the required antiviral stockpile.
神经氨酸酶抑制剂曾被用于降低 2009 年大流行性流感 A/H1N1 的传播,在 2009/2010 年大流行的早期阶段使用。各国之间和各国之内用于诊断流感以进行抗病毒干预的政策有很大差异,导致抗病毒药物使用的时机和规模不同。
方法/主要发现:利用澳大利亚社区模拟模型,确定了三种抗病毒干预策略(每种策略都包括和不包括学校停课)中,被诊断出患有症状的感染者百分比以及诊断延误的影响。根据包括繁殖数、序列间隔和特定年龄组感染率特征在内的实际数据,确定了大流行性流感 A/H1N1 的流行特征。在没有干预的情况下,根据估计的 R(0)为 1.5,确定发病率(AR)为 24.5%;仅治疗、治疗加家庭预防或治疗加家庭加延长预防的抗病毒干预分别将发病率降低至 21%、16.5%或 13%,假设诊断发生在症状出现后 24 小时,并且 50%的有症状病例被诊断。如果没有延迟进行诊断,则发病率分别降至 17%、12.2%或 8.8%。如果 90%的有症状病例被诊断(有 24 小时的延迟),则发病率分别降至 17.8%、11.1%和 7.6%。
迅速诊断出有症状的病例并诊断出较高比例的病例的能力被证明可以提高所有三种抗病毒策略的有效性。对于 R(0)<=1.5 的疫情,我们的结果表明,当病例诊断覆盖率超过约 70%时,实施延长预防策略所需的抗病毒储备量就会减少。增加至少四周的学校停课被发现可以进一步降低累计和峰值发病率以及所需抗病毒储备量。