Institut de Recherche pour le Développement (IRD), UMR 198, Rue Wagane Diouf × Georges Pompidou, Dakar, Sénégal.
Malar J. 2011 Jul 25;10:203. doi: 10.1186/1475-2875-10-203.
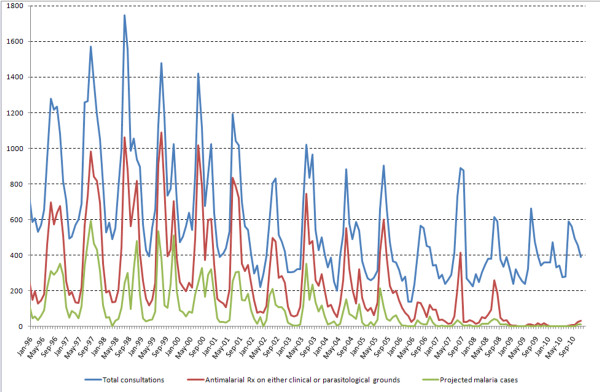
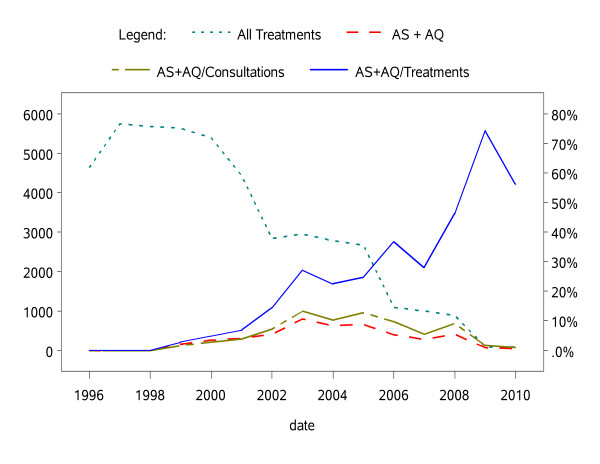
Malaria is reportedly receding in different epidemiological settings, but local long-term surveys are limited. At Mlomp dispensary in south-western Senegal, an area of moderate malaria transmission, year-round, clinically-suspected malaria was treated with monotherapy as per WHO and national policy in the 1990s. Since 2000, there has been a staggered deployment of artesunate-amodiaquine after parasitological confirmation; this was adopted nationally in 2006.
Data were extracted from clinic registers for the period between January 1996 and December 2010, analysed and modelled.
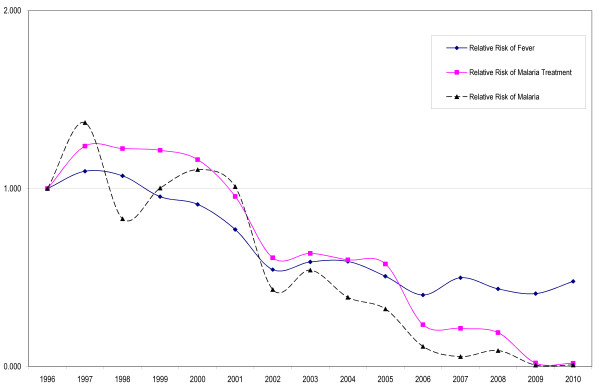
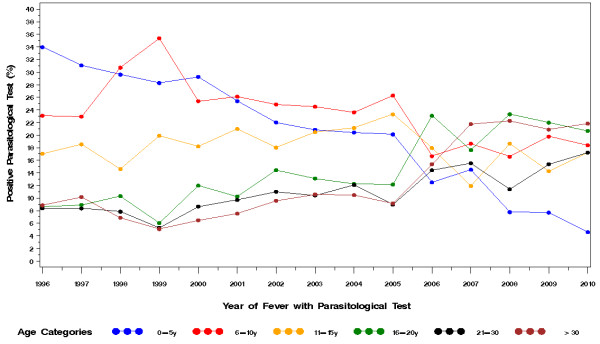
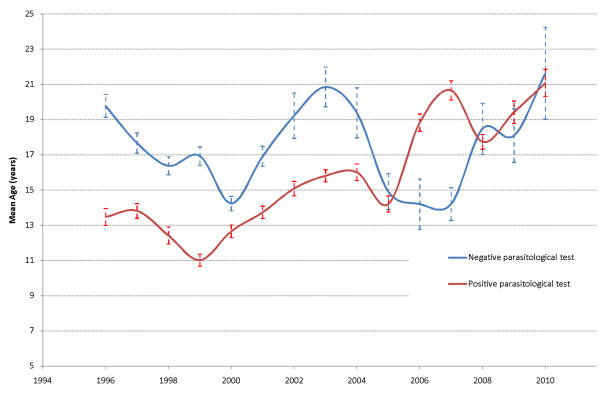
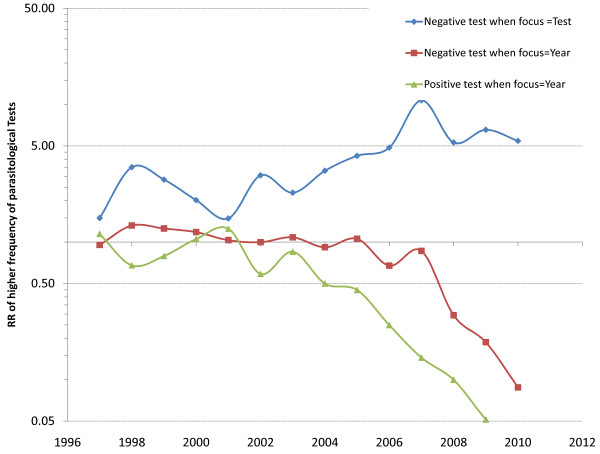
Over the 15-year study period, the risk of malaria decreased about 32-times (from 0.4 to 0.012 episodes person-year), while anti-malarial treatments decreased 13-times (from 0.9 to 0.07 treatments person-year) and consultations for fever decreased 3-times (from 1.8 to 0.6 visits person-year). This was paralleled by changes in the age profile of malaria patients so that the risk of malaria is now almost uniformly distributed throughout life, while in the past malaria used to concern more children below 16 years of age.
This study provides direct evidence of malaria risk receding between 1996-2010 and becoming equal throughout life where transmission used to be moderate. Infection rates are no longer enough to sustain immunity. Temporally, this coincides with deploying artemisinin combinations on parasitological confirmation, but other contributing causes are unclear.
据报道,疟疾在不同的流行病学环境中正在消退,但长期的本地调查有限。在塞内加尔西南部的 Mlomp 诊所,这是一个疟疾中度传播的地区,在 20 世纪 90 年代,全年按照世界卫生组织和国家政策对疑似疟疾进行单一疗法治疗。自 2000 年以来,根据寄生虫学确认结果,青蒿琥酯-阿莫地喹分阶段部署;2006 年在全国范围内采用。
从 1996 年 1 月至 2010 年 12 月的诊所登记册中提取数据,进行分析和建模。
在 15 年的研究期间,疟疾的风险降低了约 32 倍(从 0.4 降至 0.012 例/人年),而抗疟治疗降低了 13 倍(从 0.9 降至 0.07 人年),发热咨询减少了 3 倍(从 1.8 降至 0.6 人年)。这与疟疾患者年龄分布的变化相吻合,因此,疟疾的风险现在几乎均匀分布在整个生命周期中,而过去疟疾更多地发生在 16 岁以下的儿童中。
本研究提供了 1996-2010 年疟疾风险消退的直接证据,并且在传播曾经中度的地区,风险变得平等。感染率不再足以维持免疫力。从时间上看,这与在寄生虫学确认后部署青蒿素联合用药相吻合,但其他促成因素尚不清楚。