Scientific Institute for Quality of Healthcare, Radboud University Nijmegen Medical Centre, P.O. Box 9101, Nijmegen, HB 6500, The Netherlands.
BMC Fam Pract. 2012 Mar 27;13:25. doi: 10.1186/1471-2296-13-25.
International interest in pay-for-performance (P4P) initiatives to improve quality of health care is growing. Current programs vary in the methods of performance measurement, appraisal and reimbursement. One may assume that involvement of health care professionals in the goal setting and methods of quality measurement and subsequent payment schemes may enhance their commitment to and motivation for P4P programs and therefore the impact of these programs. We developed a P4P program in which the target users were involved in decisions about the P4P methods.
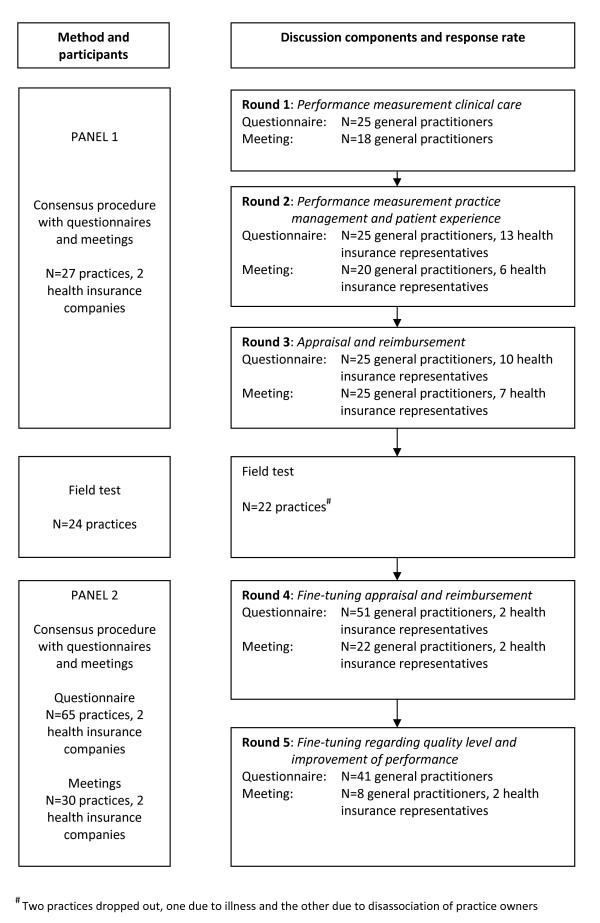
For the development of the P4P program a framework was used which distinguished three main components: performance measurement, appraisal and reimbursement. Based on this framework design choices were discussed in two panels of target users using an adapted Delphi procedure. The target users were 65 general practices and two health insurance companies in the South of the Netherlands.
Performance measurement was linked to the Dutch accreditation program based on three domains (clinical care, practice management and patient experience). The general practice was chosen as unit of assessment. Relative standards were set at the 25th percentile of group performance. The incentive for clinical care was set twice as high as the one for practice management and patient experience. Quality scores were to be calculated separately for all three domains, and for both the quality level and the improvement of performance. The incentive for quality level was set thrice as high as the one for the improvement of performance. For reimbursement, quality scores were divided into seven levels. A practice with a quality score in the lowest group was not supposed to receive a bonus. The additional payment grew proportionally for each extra group. The bonus aimed at was on average 5% to 10% of the practice income.
Designing a P4P program for primary care with involvement of the target users gave us an insight into their motives, which can help others who need to discuss similar programs. The resulting program is in line with target users' views and assessments of relevance and applicability. This may enhance their commitment to the program as was indicated by the growing number of voluntary participants after a successfully performed field test during the procedure. The elements of our framework can be very helpful for others who are developing or evaluating a P4P program.
国际上对提高医疗质量的按绩效付费(P4P)计划的兴趣日益浓厚。目前的计划在绩效衡量、评估和报销的方法上存在差异。人们可能认为,医疗保健专业人员参与目标设定以及质量衡量和随后的支付计划的方法,可以增强他们对 P4P 计划的承诺和动力,从而提高这些计划的影响力。我们制定了一项 P4P 计划,其中目标用户参与了 P4P 方法的决策。
为了制定 P4P 计划,我们使用了一个框架,该框架区分了三个主要组成部分:绩效衡量、评估和报销。基于这个框架,我们在两个目标用户小组中使用了经过修改的德尔菲程序来讨论设计选择。目标用户是荷兰南部的 65 家普通诊所和两家健康保险公司。
绩效衡量与基于三个领域(临床护理、实践管理和患者体验)的荷兰认证计划挂钩。选择普通诊所作为评估单位。相对标准设定在组绩效的第 25 百分位。临床护理的激励因素是实践管理和患者体验的两倍。质量评分将分别为所有三个领域以及绩效水平和绩效提高计算。质量水平的激励因素是绩效提高的三倍。对于报销,质量评分分为七个等级。质量评分处于最低组的诊所不应获得奖金。额外的支付将按每个额外组的比例增长。目标奖金平均为诊所收入的 5%至 10%。
在目标用户参与的情况下,为初级保健设计 P4P 计划使我们深入了解了他们的动机,这可以帮助其他需要讨论类似计划的人。由此产生的计划符合目标用户对相关性和适用性的看法和评估。这可能会增强他们对该计划的承诺,正如在程序中成功进行现场测试后自愿参与者数量的增加所表明的那样。我们框架的要素对于其他正在开发或评估 P4P 计划的人非常有帮助。