Department of Medicine, Boston University, Boston, MA, USA.
Am J Prev Med. 2012 Dec;43(6):573-83. doi: 10.1016/j.amepre.2012.08.018.
Shared decision making (SDM) is a widely recommended yet unproven strategy for increasing colorectal cancer (CRC) screening uptake. Previous trials of decision aids to increase SDM and CRC screening uptake have yielded mixed results.
To assess the impact of decision aid-assisted SDM on CRC screening uptake.
RCT.
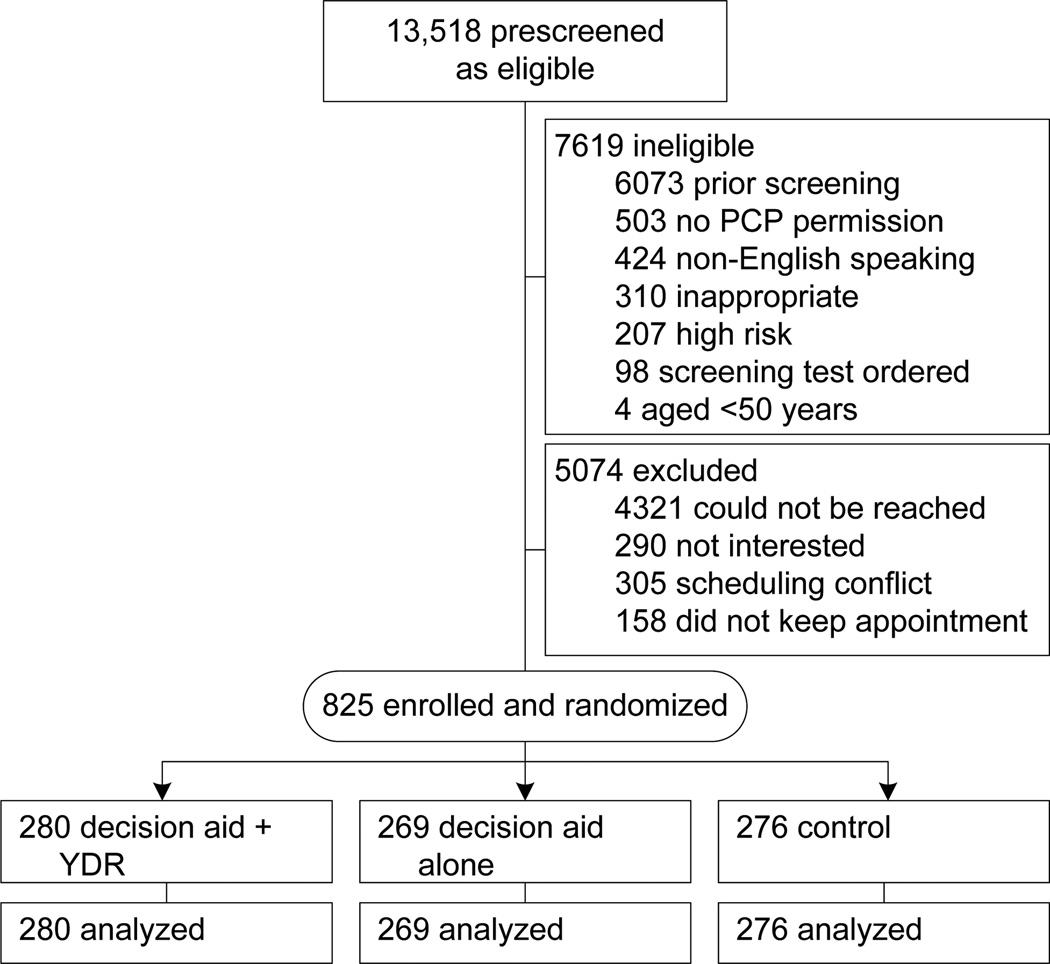
SETTING/PARTICIPANTS: The study was conducted at an urban, academic safety-net hospital and community health center between 2005 and 2010. Participants were asymptomatic, average-risk patients aged 50-75 years due for CRC screening.
Study participants (n=825) were randomized to one of two intervention arms (decision aid plus personalized risk assessment or decision aid alone) or control arm. The interventions took place just prior to a routine office visit with their primary care providers.
The primary outcome was completion of a CRC screening test within 12 months of the study visit. Logistic regression was used to identify predictors of test completion and mediators of the intervention effect. Analysis was completed in 2011.
Patients in the decision-aid group were more likely to complete a screening test than control patients (43.1% vs 34.8%, p=0.046) within 12 months of the study visit; conversely, test uptake for the decision aid and decision aid plus personalized risk assessment arms was similar (43.1% vs 37.1%, p=0.15). Assignment to the decision-aid arm (AOR=1.48, 95% CI=1.04, 2.10), black race (AOR=1.52, 95% CI=1.12, 2.06) and a preference for a patient-dominant decision-making approach (AOR=1.55, 95% CI=1.02, 2.35) were independent determinants of test completion. Activation of the screening discussion and enhanced screening intentions mediated the intervention effect.
Decision aid-assisted SDM has a modest impact on CRC screening uptake. A decision aid plus personalized risk assessment tool is no more effective than a decision aid alone.
This study is registered at www.clinicaltrials.govNCT00251862.
共同决策(SDM)是一种广泛推荐但尚未得到证实的策略,用于提高结直肠癌(CRC)筛查的参与率。以前使用决策辅助工具来增加 SDM 和 CRC 筛查参与率的试验结果喜忧参半。
评估决策辅助 SDM 对 CRC 筛查参与率的影响。
RCT。
设置/参与者:该研究于 2005 年至 2010 年在城市学术安全网医院和社区卫生中心进行。参与者为无症状、平均风险、50-75 岁的 CRC 筛查对象。
研究参与者(n=825)被随机分配到两个干预组(决策辅助加个性化风险评估或决策辅助单独)或对照组。干预措施在与初级保健提供者进行常规就诊之前进行。
主要结果是在研究就诊后 12 个月内完成 CRC 筛查测试。使用逻辑回归来确定测试完成的预测因素和干预效果的中介因素。分析于 2011 年完成。
与对照组患者(43.1% vs 34.8%,p=0.046)相比,决策辅助组患者在研究就诊后 12 个月内更有可能完成筛查测试;相反,决策辅助和决策辅助加个性化风险评估组的测试采用率相似(43.1% vs 37.1%,p=0.15)。分配到决策辅助组(AOR=1.48,95%CI=1.04,2.10)、黑种人(AOR=1.52,95%CI=1.12,2.06)和偏爱以患者为主导的决策方法(AOR=1.55,95%CI=1.02,2.35)是测试完成的独立决定因素。筛查讨论的激活和增强的筛查意图介导了干预效果。
决策辅助 SDM 对 CRC 筛查参与率有一定影响。决策辅助加个性化风险评估工具并不比决策辅助单独更有效。
本研究在 www.clinicaltrials.gov 注册,编号为 NCT00251862。