Ciaranello Andrea L, Leroy Valeriane, Rusibamayila Asinath, Freedberg Kenneth A, Shapiro Roger, Engelsmann Barbara, Lockman Shahin, Kelly Kathleen A, Dabis François, Walensky Rochelle P
aMedical Practice Evaluation Center, Division of Infectious Disease, Massachusetts General Hospital, Boston, Massachusetts, USA bUniversité Bordeaux, Institut de Santé Publique, d'Epidémiologie et de Développement (ISPED), and Centre INSERM U897-Epidemiologie-Biostatistique, Bordeaux, France cDivision of General Medicine, Massachusetts General Hospital, Boston, Massachusetts, USA dHarvard Center for AIDS Research, Boston, Massachusetts, USA eDivision of Infectious Diseases, Beth Israel Deaconess Medical Center, Boston, Massachusetts, USA fDepartment of Immunology and Infectious Diseases, Harvard School of Public Health, Boston, Massachusetts, USA gThe Botswana-Harvard School of Public Health, AIDS Institute Partnership for HIV Research and Education, Gaborone, Botswana hOrganization for Public Health Interventions and Development, Harare, Zimbabwe iDivision of Infectious Disease, Brigham and Women's Hospital, Boston, Massachusetts, USA.
AIDS. 2014 Jul;28 Suppl 3(0 3):S287-99. doi: 10.1097/QAD.0000000000000337.
To determine how infant feeding recommendations can maximize HIV-free survival (HFS) among HIV-exposed, uninfected African infants, balancing risks of breast milk-associated HIV infection with setting-specific risks of illness and death associated with replacement feeding.
Validated mathematical model of HIV-exposed, uninfected infants, with published data from Africa.
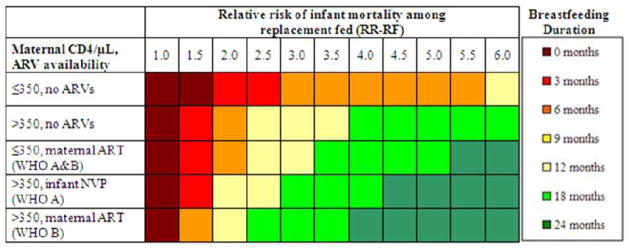
We projected 24-month HFS using combinations of: maternal CD4, antiretroviral drug availability, and relative risk of mortality among replacement-fed compared to breastfed infants ('RR-RF', range 1.0-6.0). For each combination, we identified the 'optimal' breastfeeding duration (0-24 months) maximizing HFS. We compared HFS under an 'individualized' approach, based on the above parameters, to the WHO 'public health approach' (12 months breastfeeding for all HIV-infected women).
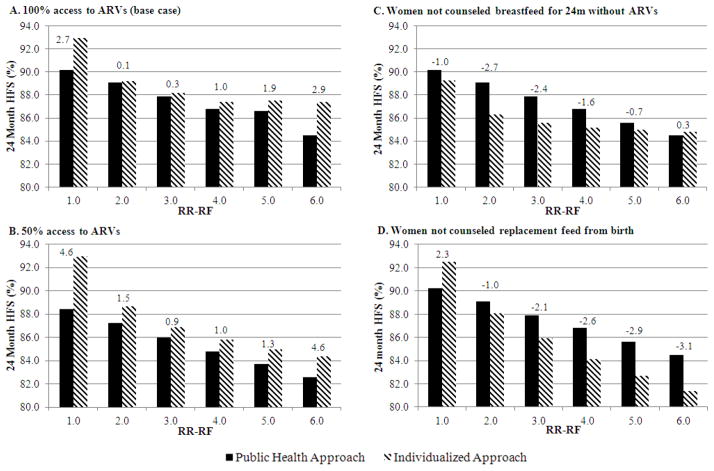
Projected HFS was 65-93%. When the value of RR-RF is 1.0, replacement feeding from birth maximized HFS. At a commonly reported RR-RF value (2.0), optimal breastfeeding duration was 3-12 months, depending on maternal CD4 and antiretroviral drug availability. As the value of RR-RF increased, optimal breastfeeding duration increased. Compared to the public health approach, an individualized approach improved absolute HFS by less than 1% if RR-RF value was 2.0-4.0, by 3% if RR-RF value was 1.0 or 6.0, and by greater amounts if access to antiretroviral drugs was limited.
Tailoring breastfeeding duration to maternal CD4, antiretroviral drug availability, and local replacement feeding safety can optimize HFS among HIV-exposed infants. An individualized approach leads to moderate gains in HFS, but only when mortality risks from replacement feeding are very low or very high, or antiretroviral drug availability is limited. The WHO public health approach is beneficial in most resource-limited settings.
确定婴儿喂养建议如何在暴露于艾滋病毒但未感染的非洲婴儿中最大化无艾滋病毒生存(HFS),平衡母乳相关艾滋病毒感染风险与特定环境下与替代喂养相关的疾病和死亡风险。
采用来自非洲的已发表数据,建立暴露于艾滋病毒但未感染婴儿的经验证数学模型。
我们使用以下组合预测24个月的无艾滋病毒生存(HFS):母亲的CD4水平、抗逆转录病毒药物的可及性,以及与母乳喂养婴儿相比,替代喂养婴儿的相对死亡风险(“RR-RF”,范围为1.0至6.0)。对于每种组合,我们确定使无艾滋病毒生存最大化的“最佳”母乳喂养持续时间(0至24个月)。我们将基于上述参数的“个性化”方法下的无艾滋病毒生存情况与世界卫生组织的“公共卫生方法”(所有感染艾滋病毒的妇女进行12个月母乳喂养)进行比较。
预测的无艾滋病毒生存为65%至93%。当RR-RF值为1.0时,从出生就进行替代喂养可使无艾滋病毒生存最大化。在常见的RR-RF值(2.0)下,最佳母乳喂养持续时间为3至12个月,具体取决于母亲的CD4水平和抗逆转录病毒药物的可及性。随着RR-RF值的增加,最佳母乳喂养持续时间也增加。与公共卫生方法相比,如果RR-RF值为2.0至4.0,个性化方法可使绝对无艾滋病毒生存提高不到1%;如果RR-RF值为1.0或6.0,可提高3%;如果抗逆转录病毒药物的可及性有限,则提高幅度更大。
根据母亲的CD4水平、抗逆转录病毒药物的可及性以及当地替代喂养的安全性来调整母乳喂养持续时间,可优化暴露于艾滋病毒婴儿的无艾滋病毒生存。个性化方法可使无艾滋病毒生存适度提高,但仅在替代喂养的死亡风险非常低或非常高,或抗逆转录病毒药物的可及性有限时才如此。世界卫生组织的公共卫生方法在大多数资源有限的环境中是有益的。