Lorem Geir Fagerjord, Schirmer Henrik, Emaus Nina
Department of caring and health science, Faculty of health sciences, The Arctic University of Norway, Tromsø, Norway.
Department of clinical medicine, Faculty of health sciences, The Arctic University of Norway, Tromsø, Norway.
PLoS One. 2016 Feb 5;11(2):e0148830. doi: 10.1371/journal.pone.0148830. eCollection 2016.
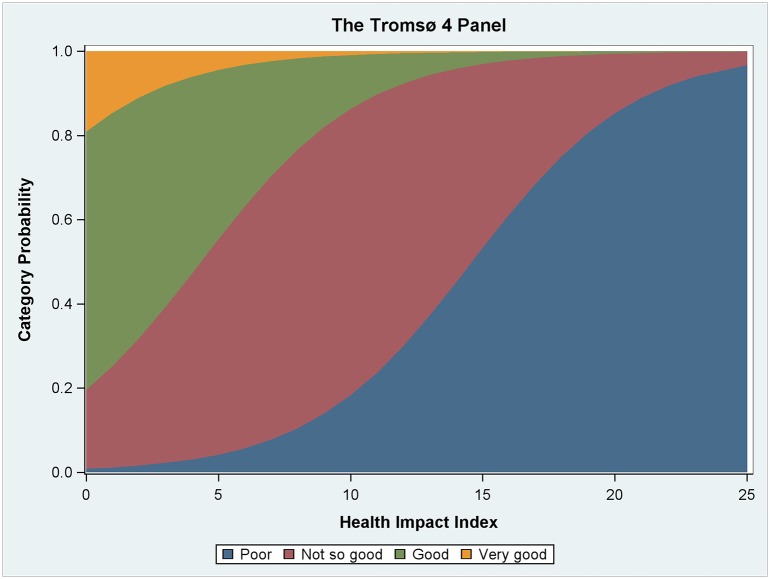
The objective of this study was to develop a method of classifying comorbid conditions that accounts for both the severity and joint effects of the diseases. The Tromsø Study is a cohort study with a longitudinal design utilizing a survey approach with physical examinations in the Tromsø municipality from 1974 to 2008, where in total 40051 subjects participated. We used Tromsø 4 as reference population and the Norwegian Institute of Public Health (FHI) panel as validation population. Ordinal regression was used to assess the effect of comorbid disease on Self-Reported Health (SRH). The model is controlled for interaction between diseases, mental health, age, and gender. The health impact index estimated levels of SRH. The comparison of predicted and observed SRH showed no significant differences. Spearman's correlation showed that increasing levels of comorbidity were related to lower levels of SRH (RS = -0.36, p <.001). The Charlson Comorbidity Index(CCI) was also associated with SRH (r = -.25, p <.001). When focusing on only individuals with a comorbid disease, the relation between SRH and the Health Impact Index (HII) was strengthened (r = -.42, p <.001), while the association between SRH and CCI was attenuated (r = -.14, p <.001). CCI was designed to control for comorbid conditions when survival/mortality is the outcome of interest but is inaccurate when the outcome is SRH. We conclude that HII should be used when SRH is not available, and well-being or quality of survival/life is the outcome of interest.
本研究的目的是开发一种对共病情况进行分类的方法,该方法要兼顾疾病的严重程度和联合效应。特罗姆瑟研究是一项队列研究,采用纵向设计,于1974年至2008年在特罗姆瑟市采用调查方法并结合体格检查,共有40051名受试者参与。我们将特罗姆瑟4作为参考人群,挪威公共卫生研究所(FHI)小组作为验证人群。采用有序回归来评估共病对自我报告健康状况(SRH)的影响。该模型对疾病之间的相互作用、心理健康、年龄和性别进行了控制。健康影响指数估算了SRH水平。预测的SRH与观察到的SRH之间的比较未显示出显著差异。斯皮尔曼相关性分析表明,共病水平的增加与较低的SRH水平相关(RS = -0.36,p <.001)。查尔森共病指数(CCI)也与SRH相关(r = -.25,p <.001)。当仅关注患有共病的个体时,SRH与健康影响指数(HII)之间的关系得到加强(r = -.42,p <.001),而SRH与CCI之间的关联减弱(r = -.14,p <.001)。CCI旨在在生存/死亡率为感兴趣的结果时控制共病情况,但当结果为SRH时并不准确。我们得出结论,当无法获得SRH,且幸福感或生存/生活质量为感兴趣的结果时,应使用HII。