Beiwinkel Till, Eißing Tabea, Telle Nils-Torge, Siegmund-Schultze Elisabeth, Rössler Wulf
Innovation Incubator, Competence Tandem Integrated Care, Leuphana University of Lüneburg, Lüneburg, Germany.
KKH Kaufmännische Krankenkasse, Abteilung Leistungs- und Versorgungsmanagement, Hannover, Germany.
J Med Internet Res. 2017 Jun 15;19(6):e213. doi: 10.2196/jmir.6546.
Depression is highly prevalent in the working population and is associated with significant loss of workdays; however, access to evidence-based treatment is limited.
This study evaluated the effectiveness of a Web-based intervention in reducing mild to moderate depression and sickness absence.
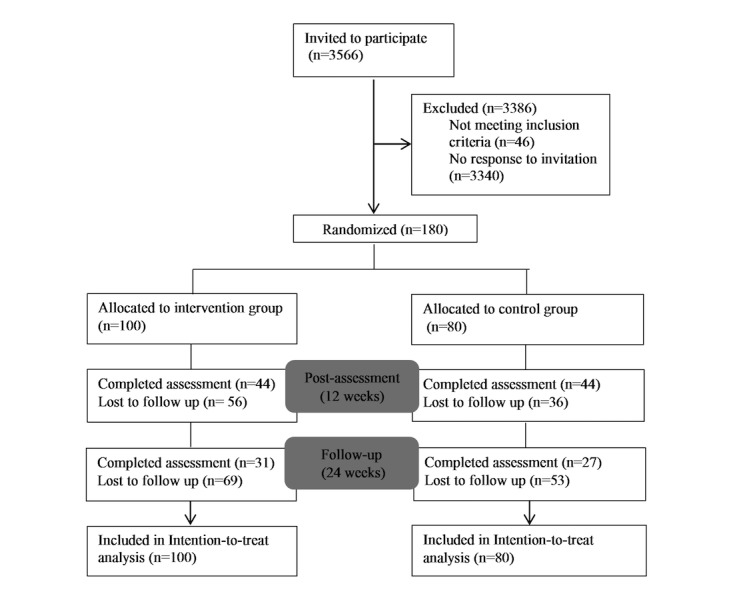
In an open-label randomized controlled trial, participants were recruited from a large-scale statutory health insurance and were assigned to two groups. The intervention group had access to a 12 week Web-based program consisting of structured interactive sessions and therapist support upon request. The wait-list control group had access to unguided Web-based psycho-education. Depressive symptoms were self-assessed at baseline, post-treatment, and follow-up (12 weeks after treatment) using the Patient Health Questionnaire (PHQ-9) and Beck Depression Inventory (BDI-II) as primary outcome measures. Data on sickness absence was retrieved from health insurance records. Intention-to-treat (ITT) analysis and per-protocol (PP) analysis were performed.
Of the 180 participants who were randomized, 88 completed the post-assessment (retention rate: 48.8%, 88/180). ITT analysis showed a significant between-group difference in depressive symptoms during post-treatment in favor of the intervention group, corresponding to a moderate effect size (PHQ-9: d=0.55, 95% CI 0.25-0.85, P<.001, and BDI-II: d=0.41, CI 0.11-0.70, P=.004). PP analysis partially supported this result, but showed a non-significant effect on one primary outcome (PHQ-9: d=0.61, 95% CI 0.15-1.07, P=.04, and BDI-II: d=0.25 95% CI -0.18 to 0.65, P=.37). Analysis of clinical significance using reliable change index revealed that significantly more participants who used the Web-based intervention (63%, 63/100) responded to the treatment versus the control group (33%, 27/80; P<.001). The number needed to treat (NNT) was 4.08. Within both groups, there was a reduction in work absence frequency (IG: -67.23%, P<.001, CG: -82.61%, P<.001), but no statistical difference in sickness absence between groups was found (P=.07).
The Web-based intervention was effective in reducing depressive symptoms among adults with sickness absence. As this trial achieved a lower power than calculated, its results should be replicated in a larger sample. Further validation of health insurance records as an outcome measure for eHealth trials is needed.
International Standard Randomized Controlled Trial Number (ISRCTN): 02446836; http://www.isrctn.com/ISRCTN02446836 (Archived by WebCite at http://www.webcitation.org/6jx4SObnw).
抑郁症在工作人群中高度流行,且与工作日的大量损失相关;然而,获得循证治疗的机会有限。
本研究评估了基于网络的干预措施在减轻轻度至中度抑郁症及减少病假方面的有效性。
在一项开放标签随机对照试验中,参与者从大规模法定医疗保险中招募,并被分为两组。干预组可使用一个为期12周的基于网络的项目,该项目包括结构化互动课程以及根据需求提供的治疗师支持。等待名单对照组可使用无指导的基于网络的心理教育。使用患者健康问卷(PHQ - 9)和贝克抑郁量表(BDI - II)作为主要结局指标,在基线、治疗后及随访(治疗后12周)时对抑郁症状进行自我评估。从医疗保险记录中获取病假数据。进行意向性分析(ITT)和符合方案分析(PP)。
在180名随机分组的参与者中,88人完成了后测(保留率:48.8%,88/180)。ITT分析显示,治疗后两组在抑郁症状方面存在显著的组间差异,干预组更具优势,对应中等效应量(PHQ - 9:d = 0.55,95%CI 0.25 - 0.85,P <.001;BDI - II:d = 0.41,CI 0.11 - 0.70,P =.004)。PP分析部分支持了这一结果,但在一个主要结局指标上显示无显著效果(PHQ - 9:d = 0.61,95%CI 0.15 - 1.07,P =.04;BDI - II:d = 0.25,95%CI -0.18至0.65,P =.37)。使用可靠变化指数进行的临床意义分析显示,与对照组(33%,27/80;P <.001)相比,使用基于网络干预措施的参与者中有显著更多比例(63%,63/100)对治疗有反应。治疗所需人数(NNT)为4.08。两组内,缺勤频率均有所降低(干预组:-67.23%,P <.001;对照组:-82.61%,P <.001),但两组间病假天数无统计学差异(P =.07)。
基于网络的干预措施在减少有病假的成年人的抑郁症状方面有效。由于本试验的效能低于计算值,其结果应在更大样本中重复验证。需要进一步验证医疗保险记录作为电子健康试验结局指标的有效性。
国际标准随机对照试验编号(ISRCTN):02446836;http://www.isrctn.com/ISRCTN02446836(由WebCite存档于http://www.webcitation.org/6jx4SObnw)