Handley Melanie, Bunn Frances, Goodman Claire
Centre for Research in Primary and Community Care, University of Hertfordshire, Hatfield, UK.
BMJ Open. 2017 Jul 16;7(7):e015257. doi: 10.1136/bmjopen-2016-015257.
To identify features of programmes and approaches to make healthcare delivery in secondary healthcare settings more dementia-friendly, providing a context-relevant understanding of how interventions achieve outcomes for people living with dementia.
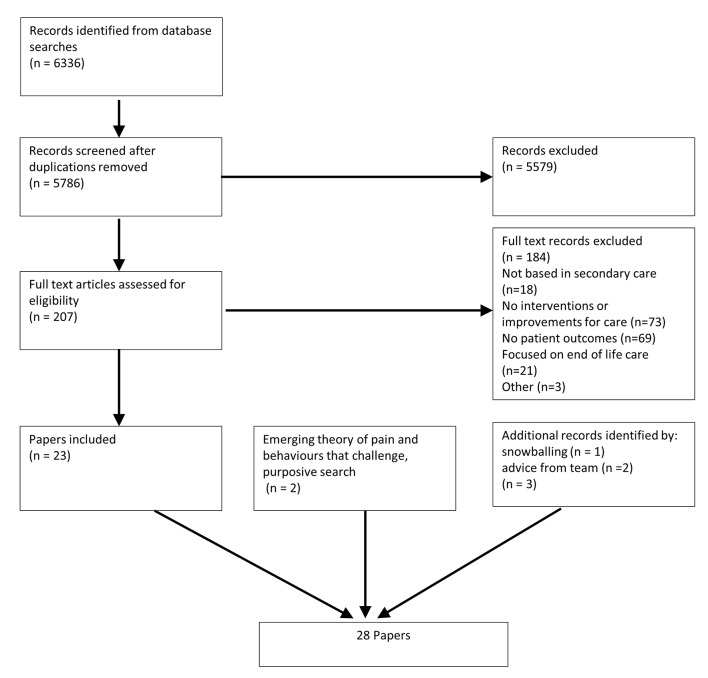
A realist review conducted in three phases: (1) stakeholder interviews and scoping of the literature to develop an initial programme theory for providing effective dementia care; (2) structured retrieval and extraction of evidence; and (3) analysis and synthesis to build and refine the programme theory.
PubMed, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Cochrane Library, NHS Evidence, Scopus and grey literature.
Studies reporting interventions and approaches to make hospital environments more dementia-friendly. Studies not reporting patient outcomes or contributing to the programme theory were excluded.
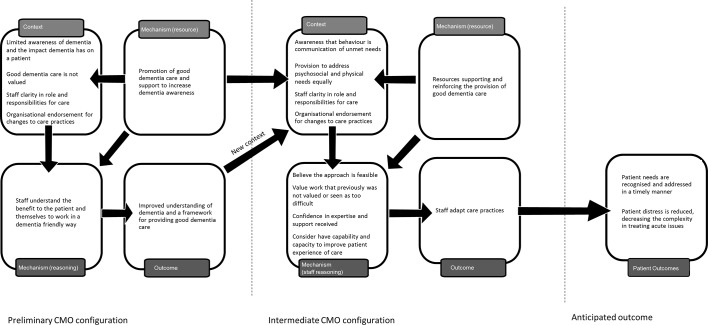
Phase 1 combined findings from 15 stakeholder interviews and 22 publications to develop candidate programme theories. Phases 2 and 3 identified and synthesised evidence from 28 publications. Prominent context-mechanism-outcome configurations were identified to explain what supported dementia-friendly healthcare in acute settings. Staff capacity to understand the behaviours of people living with dementia as communication of an unmet need, combined with a recognition and valuing of their role in their care, prompted changes to care practices. Endorsement from senior management gave staff confidence and permission to adapt working practices to provide good dementia care. Key contextual factors were the availability of staff and an alignment of ward priorities to value person-centred care approaches. A preoccupation with risk generated responses that werelikely to restrict patient choice and increase their distress.
This review suggests that strategies such as dementia awareness training alone will not improve dementia care or outcomes for patients with dementia. Instead, how staff are supported to implement learning and resources by senior team members with dementia expertise is a key component for improving care practices and patient outcomes.
CRD42015017562.
确定使二级医疗保健机构的医疗服务更有利于痴呆症患者的方案和方法的特征,提供与背景相关的理解,即干预措施如何为痴呆症患者实现预期结果。
分三个阶段进行的现实主义综述:(1)与利益相关者进行访谈并对文献进行范围界定,以制定提供有效痴呆症护理的初始方案理论;(2)对证据进行结构化检索和提取;(3)进行分析和综合,以构建和完善方案理论。
PubMed、护理及相关健康文献累积索引(CINAHL)、Cochrane图书馆、英国国家医疗服务体系证据库、Scopus以及灰色文献。
报告使医院环境更有利于痴呆症患者的干预措施和方法的研究。未报告患者结局或对方案理论无贡献的研究被排除。
第1阶段结合了15次利益相关者访谈和22篇出版物的结果,以制定候选方案理论。第2阶段和第3阶段从28篇出版物中识别并综合了证据。确定了突出的背景-机制-结果配置,以解释在急性环境中支持有利于痴呆症患者的医疗保健的因素。工作人员理解痴呆症患者行为是未满足需求的沟通的能力,再加上对他们在护理中所起作用的认可和重视,促使护理实践发生改变。高级管理层的认可给予工作人员信心和许可,使其能够调整工作实践以提供良好的痴呆症护理。关键的背景因素是工作人员的可获得性以及病房优先事项与以患者为中心的护理方法价值的一致性。对风险的过度关注产生的反应可能会限制患者的选择并增加他们的痛苦。
本综述表明,仅靠痴呆症意识培训等策略不会改善痴呆症患者的护理或结局。相反,具有痴呆症专业知识的高级团队成员如何支持工作人员实施学习内容和利用资源是改善护理实践和患者结局的关键组成部分。
CRD42015017562。