Diabetes Research Centre, University of Leicester, Leicester General Hospital, Gwendolen Rd, Leicester LE5 4PW, UK.
NIHR Leicester Biomedical Research Centre, University of Leicester, Leicester LE1 7RH, UK.
Eur Heart J. 2017 Nov 14;38(43):3232-3240. doi: 10.1093/eurheartj/ehx449.
To quantify the association of self-reported walking pace and handgrip strength with all-cause, cardiovascular, and cancer mortality.
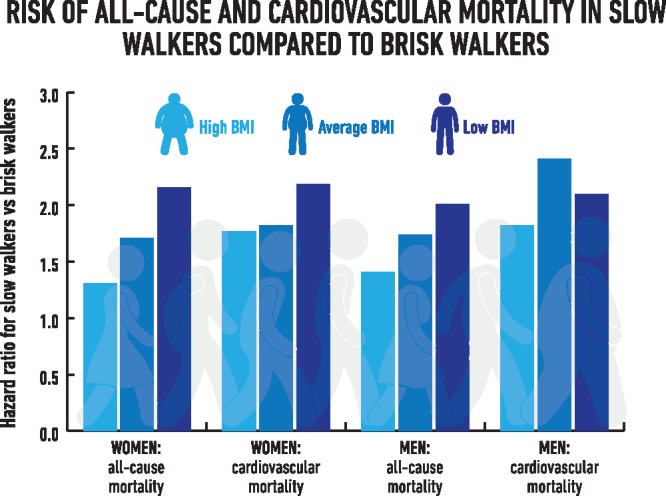
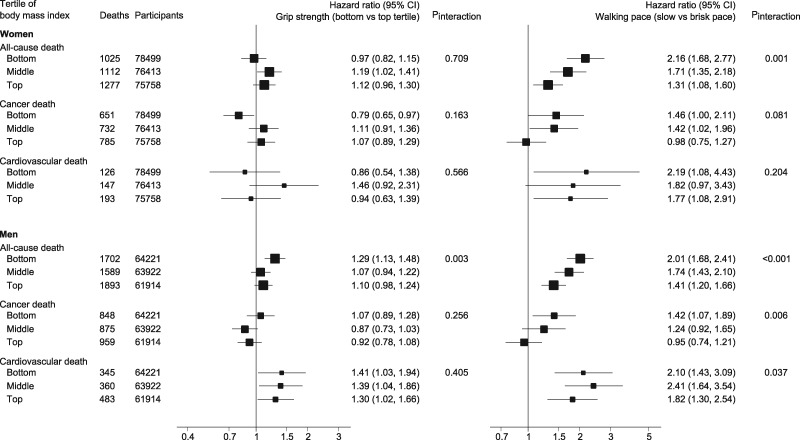
A total of 230 670 women and 190 057 men free from prevalent cancer and cardiovascular disease were included from UK Biobank. Usual walking pace was self-defined as slow, steady/average or brisk. Handgrip strength was assessed by dynamometer. Cox-proportional hazard models were adjusted for social deprivation, ethnicity, employment, medications, alcohol use, diet, physical activity, and television viewing time. Interaction terms investigated whether age, body mass index (BMI), and smoking status modified associations. Over 6.3 years, there were 8598 deaths, 1654 from cardiovascular disease and 4850 from cancer. Associations of walking pace with mortality were modified by BMI. In women, the hazard ratio (HR) for all-cause mortality in slow compared with fast walkers were 2.16 [95% confidence interval (CI): 1.68-2.77] and 1.31 (1.08-1.60) in the bottom and top BMI tertiles, respectively; corresponding HRs for men were 2.01 (1.68-2.41) and 1.41 (1.20-1.66). Hazard ratios for cardiovascular mortality remained above 1.7 across all categories of BMI in men and women, with modest heterogeneity in men. Handgrip strength was associated with cardiovascular mortality in men only (HR tertile 1 vs. tertile 3 = 1.38; 1.18-1.62), without differences across BMI categories, while associations with all-cause mortality were only seen in men with low BMI. Associations for walking pace and handgrip strength with cancer mortality were less consistent.
A simple self-reported measure of slow walking pace could aid risk stratification for all-cause and cardiovascular mortality within the general population.
定量评估自我报告的行走速度和握力与全因、心血管疾病和癌症死亡率的相关性。
本研究共纳入了来自英国生物银行的 230670 名女性和 190057 名无现有癌症和心血管疾病的男性。通常的行走速度由自我定义为缓慢、稳定/平均或轻快。握力通过测力计进行评估。Cox 比例风险模型调整了社会剥夺、种族、就业、药物使用、饮酒、饮食、体力活动和看电视时间。交互项研究了年龄、体重指数(BMI)和吸烟状况是否改变了相关性。在 6.3 年的随访期间,共有 8598 人死亡,1654 人死于心血管疾病,4850 人死于癌症。行走速度与死亡率的相关性受 BMI 影响。在女性中,与快速行走者相比,缓慢行走者的全因死亡率的危险比(HR)分别在 BMI 最低和最高三分位组中为 2.16(95%置信区间[CI]:1.68-2.77)和 1.31(1.08-1.60);男性相应的 HR 分别为 2.01(1.68-2.41)和 1.41(1.20-1.66)。在男性和女性中,所有 BMI 类别中心血管疾病死亡率的 HR 均高于 1.7,男性中存在适度的异质性。握力仅与男性的心血管疾病死亡率相关(第 1 三分位与第 3 三分位相比 HR=1.38;1.18-1.62),而与 BMI 类别无关,而与全因死亡率的相关性仅见于低 BMI 的男性。行走速度和握力与癌症死亡率的相关性不太一致。
简单的自我报告的缓慢行走速度可以帮助一般人群进行全因和心血管疾病死亡率的风险分层。