Burnim Michael, Ivy Julianne A, King Charles H
Center for Global Health and Diseases and WHO Collaborating Centre for Research and Training for Schistosomiasis Elimination, Case Western Reserve University School of Medicine, Cleveland, Ohio, United States of America.
Schistosomiasis Consortium for Operational Research and Evaluation, University of Georgia, Athens, Georgia, United States of America.
PLoS Negl Trop Dis. 2017 Oct 27;11(10):e0006043. doi: 10.1371/journal.pntd.0006043. eCollection 2017 Oct.
The mainstay of current schistosomiasis control programs is mass preventive chemotherapy of school-aged children with praziquantel. This treatment is delivered through school-based, community-based, or combined school- and community-based systems. Attaining very high coverage rates for children is essential in mass schistosomiasis treatment programs, as is ensuring that there are no persistently untreated subpopulations, a potential challenge for school-based programs in areas with low school enrollment. This review sought to compare the different treatment delivery methods based both on their coverage of school-aged children overall and on their coverage specifically of non-enrolled children. In addition, qualitative community or programmatic factors associated with high or low coverage rates were identified, with suggestions for overall coverage improvement.
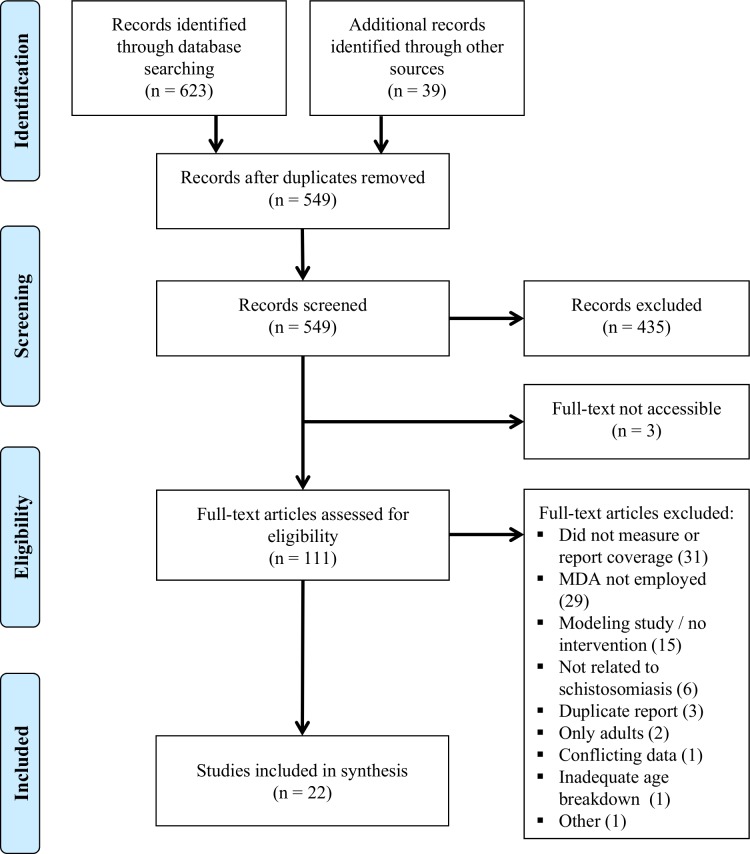
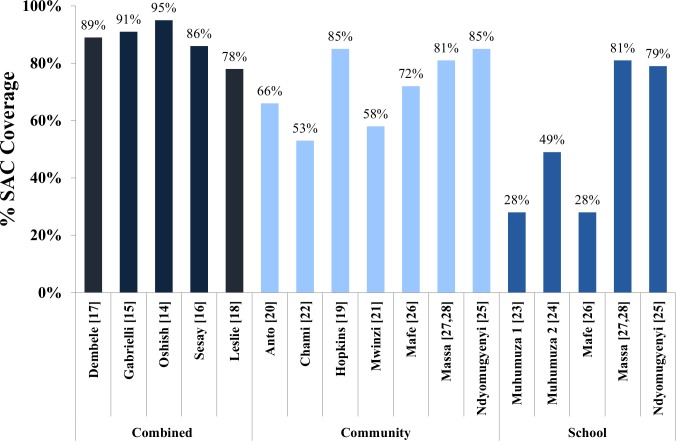
METHODOLOGY/PRINCIPAL FINDINGS: This review was registered prospectively with PROSPERO (CRD 42015017656). Five hundred forty-nine publication of potential relevance were identified through database searches, reference lists, and personal communications. Eligible studies included those published before October 2015, written in English or French, containing quantitative or qualitative data about coverage rates for MDA of school-aged children with praziquantel. Among the 22 selected studies, combined community- and school-based programs achieved the highest median coverage rates (89%), followed by community-based programs (72%). School-based programs had both the lowest median coverage of children overall (49%) and the lowest coverage of the non-enrolled subpopulation of children. Qualitatively, major factors affecting program success included fear of side effects, inadequate education about schistosomiasis, lack of incentives for drug distributors, and inequitable distribution to minority groups.
CONCLUSIONS/SIGNIFICANCE: This review provides an evidence-based framework for the development of future schistosomiasis control programs. Based on our results, a combined community and school-based delivery system should maximize coverage for both in- and out-of-school children, especially when combined with interventions such as snacks for treated children, educational campaigns, incentives for drug distributors, and active inclusion of marginalized groups.
ClinicalTrials.gov CRD42015017656.
当前血吸虫病控制项目的主要手段是对学龄儿童采用吡喹酮进行群体预防性化疗。这种治疗通过基于学校、基于社区或学校与社区相结合的系统来实施。在大规模血吸虫病治疗项目中,实现极高的儿童覆盖率至关重要,确保不存在持续未接受治疗的亚人群同样重要,这对于入学率低的地区基于学校的项目而言是一个潜在挑战。本综述旨在比较不同的治疗实施方法,既基于其对学龄儿童的总体覆盖率,也基于其对未入学儿童的具体覆盖率。此外,还确定了与高覆盖率或低覆盖率相关的定性社区或项目因素,并提出了提高总体覆盖率的建议。
方法/主要发现:本综述已在PROSPERO(CRD 42015017656)上进行了前瞻性注册。通过数据库检索、参考文献列表和个人交流,共识别出549篇可能相关的出版物。符合条件的研究包括2015年10月之前发表的、用英语或法语撰写的、包含关于学龄儿童吡喹酮大规模药物治疗覆盖率的定量或定性数据的研究。在所选的22项研究中,社区与学校相结合的项目实现了最高的中位数覆盖率(89%),其次是基于社区的项目(72%)。基于学校的项目在儿童总体中位数覆盖率方面最低(49%),在未入学儿童亚人群覆盖率方面也最低。从定性角度来看,影响项目成功的主要因素包括对副作用的恐惧、对血吸虫病的教育不足、对药物分发者缺乏激励以及对少数群体的不公平分配。
结论/意义:本综述为未来血吸虫病控制项目的发展提供了一个基于证据的框架。根据我们的研究结果,社区与学校相结合的实施系统应能最大限度地提高在校儿童和校外儿童的覆盖率,特别是当与诸如为接受治疗的儿童提供零食、开展教育活动、对药物分发者提供激励以及积极纳入边缘化群体等干预措施相结合时。
ClinicalTrials.gov CRD42015017656。