Ward Tonya L, Dominguez-Bello Maria Gloria, Heisel Tim, Al-Ghalith Gabriel, Knights Dan, Gale Cheryl A
BioTechnology Institute, University of Minnesota, St. Paul, Minnesota, USA.
Departments of Biochemistry and Microbiology and Anthropology, Rutgers University, New Brunswick, New Jersey, USA.
mSystems. 2018 Mar 6;3(3). doi: 10.1128/mSystems.00140-17. eCollection 2018 May-Jun.
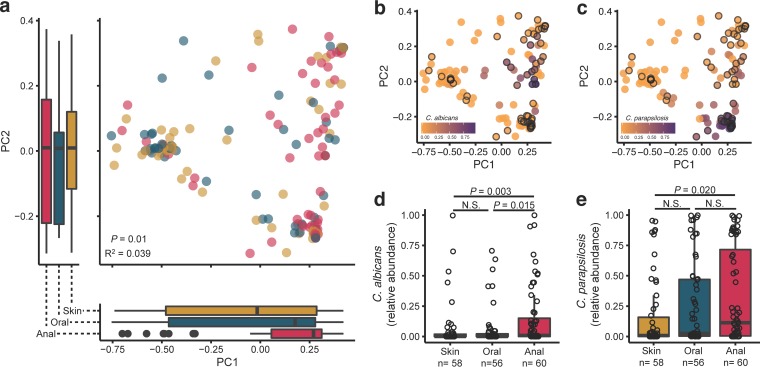
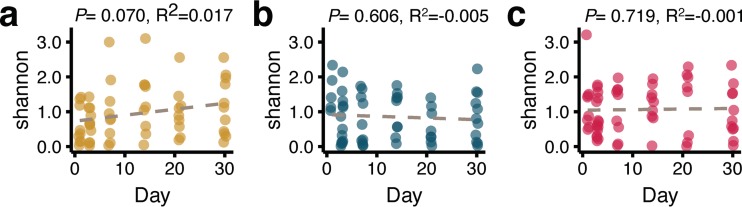
With the advent of next-generation sequencing and microbial community characterization, we are beginning to understand the key factors that shape early-life microbial colonization and associated health outcomes. Studies characterizing infant microbial colonization have focused mostly on bacteria in the microbiome and have largely neglected fungi (the mycobiome), despite their relevance to mucosal infections in healthy infants. In this pilot study, we characterized the skin, oral, and anal mycobiomes of infants over the first month of life ( = 17) and the anal and vaginal mycobiomes of mothers ( = 16) by internal transcribed spacer 2 (ITS2) amplicon sequencing. We found that infant mycobiomes differed by body site, with the infant mycobiomes at the anal sites being different from those at the skin and oral sites. The relative abundances of body site-specific taxa differed by birth mode, with significantly more fungi present on the skin of vaginally born infants on day 30 and significantly more fungi present in the oral cavity of caesarean section-born infants throughout the first month of life. We found the mycobiomes within individual infants to be variable over the first month of life, and vaginal birth did not result in infant mycobiomes that were more similar to the mother's vaginal mycobiome. Therefore, although vertical transmission of specific fungal isolates from mother to infant has been reported, it is likely that other sources (environment, other caregivers) also contribute to early-life mycobiome establishment. Thus, future longitudinal studies of mycobiome and bacterial microbiome codevelopment, with dense sampling from birth to beyond the first month of life, are warranted. Humans are colonized by diverse fungi (mycobiome), which have received much less study to date than colonizing bacteria. We know very little about the succession of fungal colonization in early life and whether it may relate to long-term health. To better understand fungal colonization and its sources, we studied the skin, oral, and anal mycobiomes of healthy term infants and the vaginal and anal mycobiomes of their mothers. Generally, infants were colonized by few fungal taxa, and fungal alpha diversity did not increase over the first month of life. There was no clear community maturation over the first month of life, regardless of body site. Key body-site-specific taxa, but not overall fungal community structures, were impacted by birth mode. Thus, additional studies to characterize mycobiome acquisition and succession throughout early life are needed to form a foundation for research into the relationship between mycobiome development and human disease.
随着下一代测序技术的出现以及微生物群落特征分析技术的发展,我们开始了解塑造早期微生物定植及相关健康结果的关键因素。尽管真菌(真菌群落)与健康婴儿的黏膜感染相关,但表征婴儿微生物定植的研究大多集中在微生物组中的细菌,而在很大程度上忽视了真菌。在这项试点研究中,我们通过内转录间隔区2(ITS2)扩增子测序,对出生后第一个月内婴儿(n = 17)的皮肤、口腔和肛门真菌群落以及母亲(n = 16)的肛门和阴道真菌群落进行了表征。我们发现婴儿真菌群落因身体部位而异,肛门部位的婴儿真菌群落与皮肤和口腔部位的不同。特定身体部位分类群的相对丰度因分娩方式而异,在出生后第30天,阴道分娩的婴儿皮肤上存在显著更多的马拉色菌属真菌,在整个出生后的第一个月内,剖宫产出生的婴儿口腔中存在显著更多的念珠菌属真菌。我们发现个体婴儿在出生后的第一个月内真菌群落是可变的,并且阴道分娩并未导致婴儿真菌群落与母亲的阴道真菌群落更相似。因此,尽管已有报道特定真菌菌株可从母亲垂直传播给婴儿,但其他来源(环境、其他照顾者)也可能对早期真菌群落的建立有贡献。因此,有必要开展未来的纵向研究,对真菌群落和细菌微生物群落的共同发育进行研究,从出生到出生后第一个月进行密集采样。人类被多种真菌(真菌群落)定植,与定植细菌相比,真菌群落迄今受到的研究要少得多。我们对早期生命中真菌定植的演替以及它是否可能与长期健康有关了解甚少。为了更好地理解真菌定植及其来源,我们研究了健康足月儿的皮肤、口腔和肛门真菌群落以及他们母亲的阴道和肛门真菌群落。一般来说,婴儿被很少的真菌分类群定植,并且真菌α多样性在出生后的第一个月内没有增加。在出生后的第一个月内,无论身体部位如何,都没有明显的群落成熟现象。分娩方式影响关键的身体部位特异性分类群,但不影响整体真菌群落结构。因此,需要开展更多研究来表征整个早期生命中真菌群落的获得和演替,为研究真菌群落发育与人类疾病之间的关系奠定基础。