Bock Jelena, Töger Johannes, Bidhult Sebastian, Markenroth Bloch Karin, Arvidsson Per, Kanski Mikael, Arheden Håkan, Testud Frederik, Greiser Andreas, Heiberg Einar, Carlsson Marcus
1 Department of Clinical Sciences, Lund University, Clinical Physiology, Skåne University Hospital, Lund, Sweden.
2 Department of Diagnostic Radiology, Lund University, Skåne University Hospital, Lund, Sweden.
Acta Radiol. 2019 Mar;60(3):327-337. doi: 10.1177/0284185118784981. Epub 2018 Jun 26.
4D-flow magnetic resonance imaging (MRI) is increasingly used.
To validate 4D-flow sequences in phantom and in vivo, comparing volume flow and kinetic energy (KE) head-to-head, with and without respiratory gating.
Achieva dStream (Philips Healthcare) and MAGNETOM Aera (Siemens Healthcare) 1.5-T scanners were used. Phantom validation measured pulsatile, three-dimensional flow with 4D-flow MRI and laser particle imaging velocimetry (PIV) as reference standard. Ten healthy participants underwent three cardiac MRI examinations each, consisting of cine-imaging, 2D-flow (aorta, pulmonary artery), and 2 × 2 accelerated 4D-flow with (Resp+) and without (Resp-) respiratory gating. Examinations were acquired consecutively on both scanners and one examination repeated within two weeks. Volume flow in the great vessels was compared between 2D- and 4D-flow. KE were calculated for all time phases and voxels in the left ventricle.
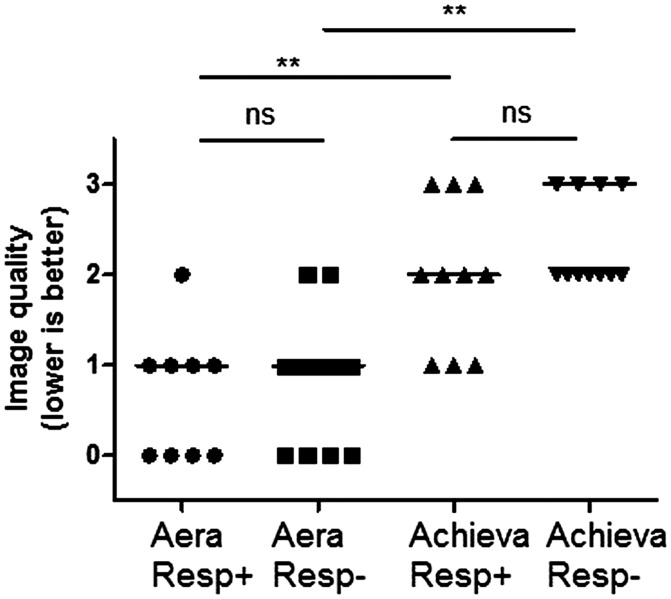
Phantom results showed high accuracy and precision for both scanners. In vivo, higher accuracy and precision ( P < 0.001) was found for volume flow for the Aera prototype with Resp+ (-3.7 ± 10.4 mL, r = 0.89) compared to the Achieva product sequence (-17.8 ± 18.6 mL, r = 0.56). 4D-flow Resp- on Aera had somewhat larger bias (-9.3 ± 9.6 mL, r = 0.90) compared to Resp+ ( P = 0.005). KE measurements showed larger differences between scanners on the same day compared to the same scanner at different days.
Sequence-specific in vivo validation of 4D-flow is needed before clinical use. 4D-flow with the Aera prototype sequence with a clinically acceptable acquisition time (<10 min) showed acceptable bias in healthy controls to be considered for clinical use. Intra-individual KE comparisons should use the same sequence.
四维血流磁共振成像(MRI)的应用日益广泛。
在体模和体内验证四维血流序列,在有和没有呼吸门控的情况下,直接比较容积流量和动能(KE)。
使用了飞利浦医疗的Achieva dStream和西门子医疗的MAGNETOM Aera 1.5-T扫描仪。体模验证采用四维血流MRI测量脉动三维血流,并以激光粒子成像测速技术(PIV)作为参考标准。10名健康受试者每人接受了三次心脏MRI检查,包括电影成像、二维血流(主动脉、肺动脉)以及有(Resp+)和无(Resp-)呼吸门控的2×2加速四维血流检查。在两台扫描仪上连续进行检查,且在两周内重复一次检查。比较二维血流和四维血流中大血管的容积流量。计算左心室所有时间相位和体素的动能。
体模结果显示两台扫描仪均具有较高的准确性和精密度。在体内,与Achieva产品序列(-17.8±18.6 mL,r = 0.56)相比,配备Resp+的Aera原型机在容积流量方面具有更高的准确性和精密度(P < 0.001,-3.7±10.4 mL,r = 0.89)。与Resp+相比,Aera上的四维血流Resp-偏差稍大(-9.3±9.6 mL,r = 0.90,P = 0.005)。与同一台扫描仪在不同日期相比,同一天不同扫描仪之间的动能测量差异更大。
在临床应用前,需要对四维血流进行特定序列的体内验证。配备临床可接受采集时间(<10分钟)的Aera原型序列的四维血流在健康对照中显示出可接受的偏差,可考虑用于临床。个体内的动能比较应使用相同序列。