Dipartimento di Fisiopatologia Medico-Chirurgica e dei Trapianti, Università degli Studi di Milano, A.O. San Paolo - Polo Universitario, Via A. Di Rudinì, 8, 20142, Milano, Italy.
SC Anestesia e Rianimazione, ASST Santi Paolo e Carlo, Ospedale San Paolo - Polo Universitario, Milano, Italy.
Crit Care. 2019 Jan 7;23(1):3. doi: 10.1186/s13054-018-2280-x.
ICU patients must be kept conscious, calm, and cooperative even during the critical phases of illness. Enteral administration of sedative drugs might avoid over sedation, and would be as adequate as intravenous administration in patients who are awake, with fewer side effects and lower costs. This study compares two sedation strategies, for early achievement and maintenance of the target light sedation.
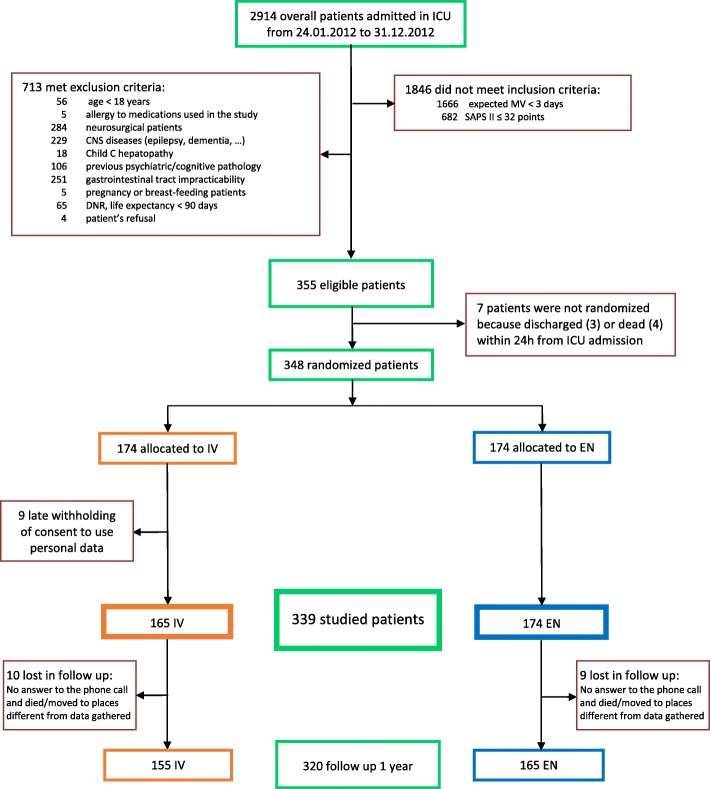
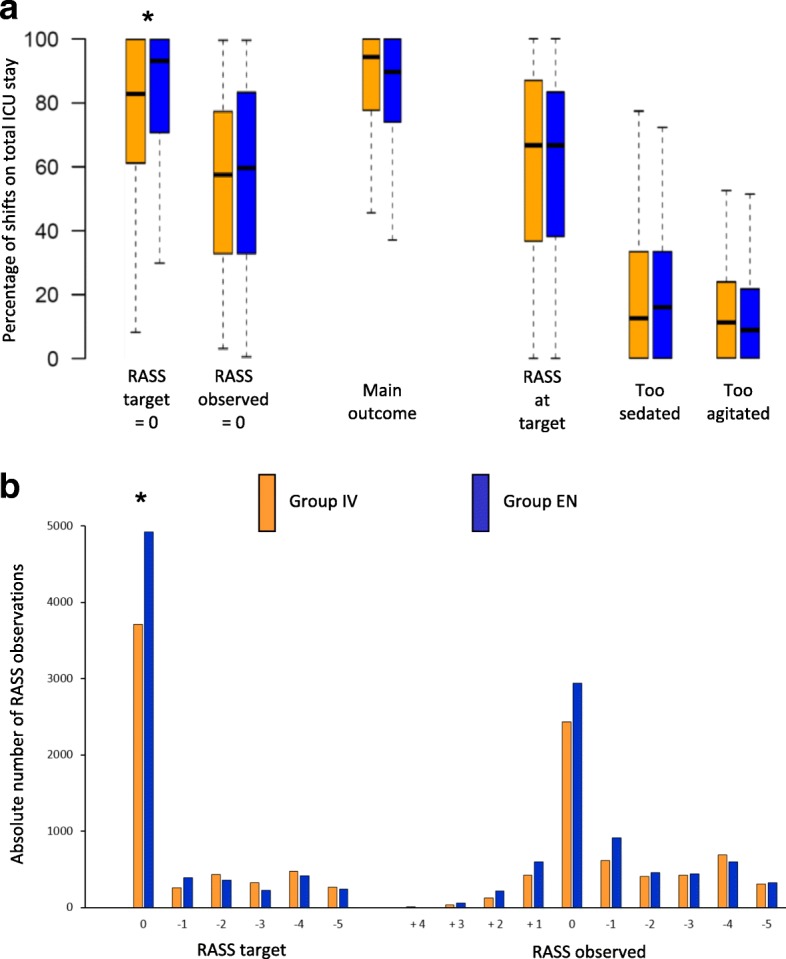
This was a multicenter, single-blind, randomized and controlled trial carried out in 12 Italian ICUs, involving patients with expected mechanical ventilation duration > 72 h at ICU admission and predicted mortality > 12% (Simplified Acute Physiology Score II > 32 points) during the first 24 h on ICU. Patients were randomly assigned to receive intravenous (midazolam, propofol) or enteral (hydroxyzine, lorazepam, and melatonin) sedation. The primary outcome was percentage of work shifts with the patient having an observed Richmond Agitation-Sedation Scale (RASS) = target RASS ±1. Secondary outcomes were feasibility, delirium-free and coma-free days, costs of drugs, length of ICU and hospital stay, and ICU, hospital, and one-year mortality.
There were 348 patients enrolled. There were no differences in the primary outcome: enteral 89.8% (74.1-100), intravenous 94.4% (78-100), p = 0.20. Enteral-treated patients had more protocol violations: n = 81 (46.6%) vs 7 (4.2%), p < 0.01; more self-extubations: n = 14 (8.1%) vs 4 (2.4%), p = 0.03; a lighter sedative target (RASS = 0): 93% (71-100) vs 83% (61-100), p < 0.01; and lower total drug costs: 2.39 (0.75-9.78) vs 4.15 (1.20-20.19) €/day with mechanical ventilation (p = 0.01).
Although enteral sedation of critically ill patients is cheaper and permits a lighter sedation target, it is not superior to intravenous sedation for reaching the RASS target.
ClinicalTrials.gov, NCT01360346 . Registered on 25 March 2011.
即使在疾病的关键阶段,ICU 患者也必须保持清醒、镇静和合作。肠内给予镇静药物可能避免过度镇静,并且对于清醒患者与静脉给予镇静药物同样有效,具有更少的副作用和更低的成本。这项研究比较了两种镇静策略,以早期达到并维持目标浅镇静。
这是一项在意大利 12 家 ICU 进行的多中心、单盲、随机对照试验,纳入预计 ICU 入住时机械通气时间>72 小时和预计入住 ICU 24 小时内死亡率>12%(简化急性生理学评分 II >32 分)的患者。患者被随机分配接受静脉(咪达唑仑、丙泊酚)或肠内(羟嗪、劳拉西泮和褪黑素)镇静。主要结局为患者观察到的 Richmond 躁动-镇静量表(RASS)=目标 RASS ±1 的工作班次比例。次要结局为可行性、无谵妄和无昏迷天数、药物成本、ICU 和住院时间以及 ICU、医院和 1 年死亡率。
共纳入 348 例患者。主要结局无差异:肠内 89.8%(74.1-100),静脉 94.4%(78-100),p=0.20。肠内治疗组的方案违反更多:n=81(46.6%)vs 7(4.2%),p<0.01;自我拔管更多:n=14(8.1%)vs 4(2.4%),p=0.03;镇静目标更轻(RASS=0):93%(71-100)vs 83%(61-100),p<0.01;机械通气时总药物费用更低:2.39(0.75-9.78)vs 4.15(1.20-20.19)€/天(p=0.01)。
尽管危重症患者的肠内镇静更便宜且允许更轻的镇静目标,但在达到 RASS 目标方面并不优于静脉镇静。
ClinicalTrials.gov,NCT01360346。于 2011 年 3 月 25 日注册。