Department of Anesthesiology and Critical Care, Perelman School of Medicine at the University of Pennsylvania, Philadelphia, Pennsylvania, United States of America.
Department of Biomedical and Health Informatics, Children's Hospital of Philadelphia, Philadelphia, Pennsylvania, United States of America.
PLoS One. 2019 Feb 22;14(2):e0212665. doi: 10.1371/journal.pone.0212665. eCollection 2019.
Rapid antibiotic administration is known to improve sepsis outcomes, however early diagnosis remains challenging due to complex presentation. Our objective was to develop a model using readily available electronic health record (EHR) data capable of recognizing infant sepsis at least 4 hours prior to clinical recognition.
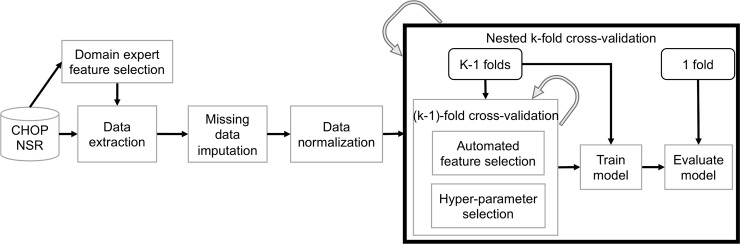
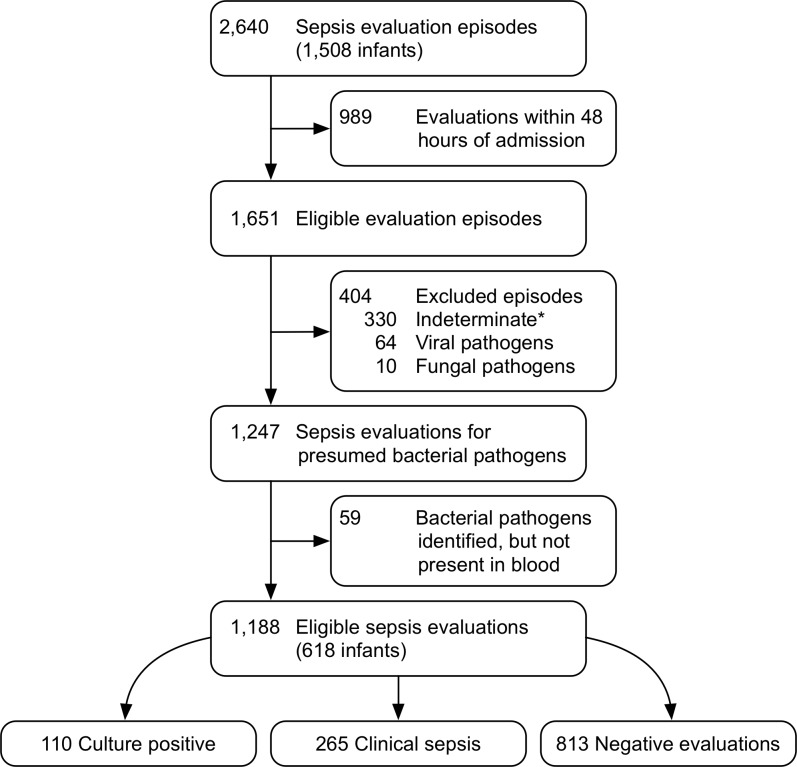
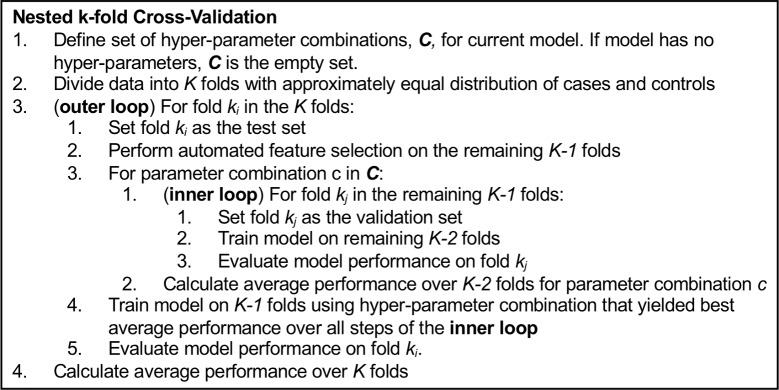
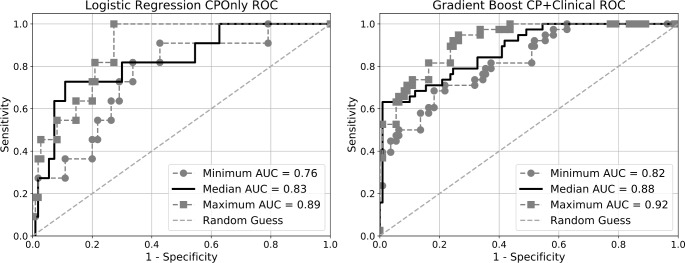
We performed a retrospective case control study of infants hospitalized ≥48 hours in the Neonatal Intensive Care Unit (NICU) at the Children's Hospital of Philadelphia between September 2014 and November 2017 who received at least one sepsis evaluation before 12 months of age. We considered two evaluation outcomes as cases: culture positive-positive blood culture for a known pathogen (110 evaluations); and clinically positive-negative cultures but antibiotics administered for ≥120 hours (265 evaluations). Case data was taken from the 44-hour window ending 4 hours prior to evaluation. We randomly sampled 1,100 44-hour windows of control data from all times ≥10 days removed from any evaluation. Model inputs consisted of up to 36 features derived from routine EHR data. Using 10-fold nested cross-validation, 8 machine learning models were trained to classify inputs as sepsis positive or negative. When tasked with discriminating culture positive cases from controls, 6 models achieved a mean area under the receiver operating characteristic (AUC) between 0.80-0.82 with no significant differences between them. Including both culture and clinically positive cases, the same 6 models achieved an AUC between 0.85-0.87, again with no significant differences.
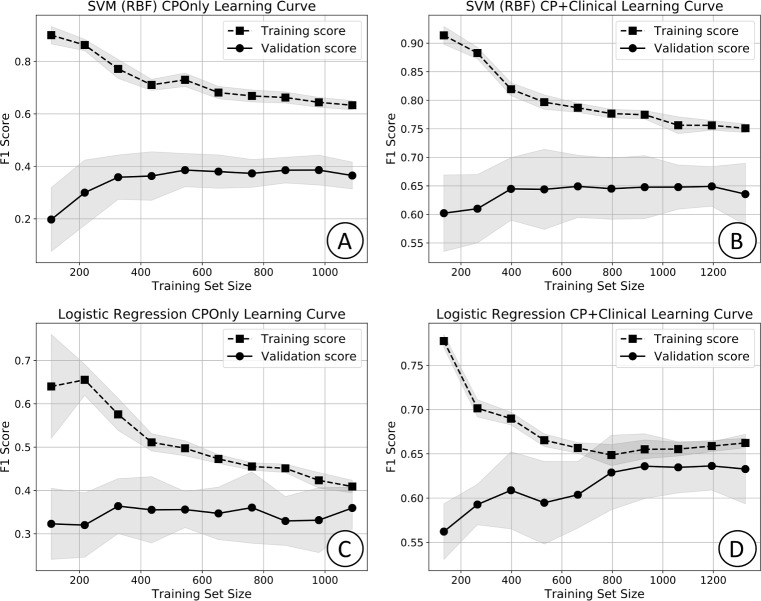
Machine learning models can identify infants with sepsis in the NICU hours prior to clinical recognition. Learning curves indicate model improvement may be achieved with additional training examples. Additional input features may also improve performance. Further research is warranted to assess potential performance improvements and clinical efficacy in a prospective trial.
快速给予抗生素已被证实可以改善脓毒症的结局,但由于其临床表现复杂,早期诊断仍然具有挑战性。我们的目标是利用易于获取的电子健康记录(EHR)数据开发一种模型,使其能够在临床识别之前至少 4 小时识别婴儿脓毒症。
我们对 2014 年 9 月至 2017 年 11 月期间在费城儿童医院新生儿重症监护病房(NICU)住院时间≥48 小时且在 12 个月龄之前至少接受过一次脓毒症评估的婴儿进行了回顾性病例对照研究。我们将两种评估结果作为病例:培养阳性-阳性血培养出已知病原体(110 次评估);以及临床阳性-阴性培养但抗生素使用≥120 小时(265 次评估)。病例数据取自评估前 4 小时结束的 44 小时窗口。我们从所有≥10 天且与任何评估均无关联的时间中随机抽取了 1100 个 44 小时窗口的对照数据。模型输入由来自常规 EHR 数据的最多 36 个特征组成。使用 10 折嵌套交叉验证,对 8 个机器学习模型进行了训练,以将输入分类为脓毒症阳性或阴性。当任务是将培养阳性病例与对照区分开来时,6 个模型的平均接受者操作特征(ROC)曲线下面积(AUC)在 0.80-0.82 之间,它们之间没有显著差异。包括培养和临床阳性病例在内,相同的 6 个模型的 AUC 在 0.85-0.87 之间,也没有显著差异。
机器学习模型可以在临床识别之前数小时识别 NICU 中的脓毒症婴儿。学习曲线表明,随着更多的训练示例,模型的改进可能会实现。更多的输入特征也可能会提高性能。需要进一步的研究来评估在前瞻性试验中的潜在性能改进和临床疗效。