Jouan Youenn, Grammatico-Guillon Leslie, Teixera Noémie, Hassen-Khodja Claire, Gaborit Christophe, Salmon-Gandonnière Charlotte, Guillon Antoine, Ehrmann Stephan
Service de Médecine Intensive Réanimation, CHRU de Tours, 2 Bd Tonnellé, 37044, Tours Cedex 9, France.
INSERM U1100 Centre d'Etudes des Pathologies Respiratoires, Faculté de Médecine, Tours, France.
Ann Intensive Care. 2019 Nov 9;9(1):126. doi: 10.1186/s13613-019-0599-3.
The post intensive care syndrome (PICS) gathers various disabilities, associated with a substantial healthcare use. However, patients' comorbidities and active medical conditions prior to intensive care unit (ICU) admission may partly drive healthcare use after ICU discharge. To better understand retative contribution of critical illness and PICS-compared to pre-existing comorbidities-as potential determinant of post-critical illness healthcare use, we conducted a population-based evaluation of patients' healthcare use trajectories.
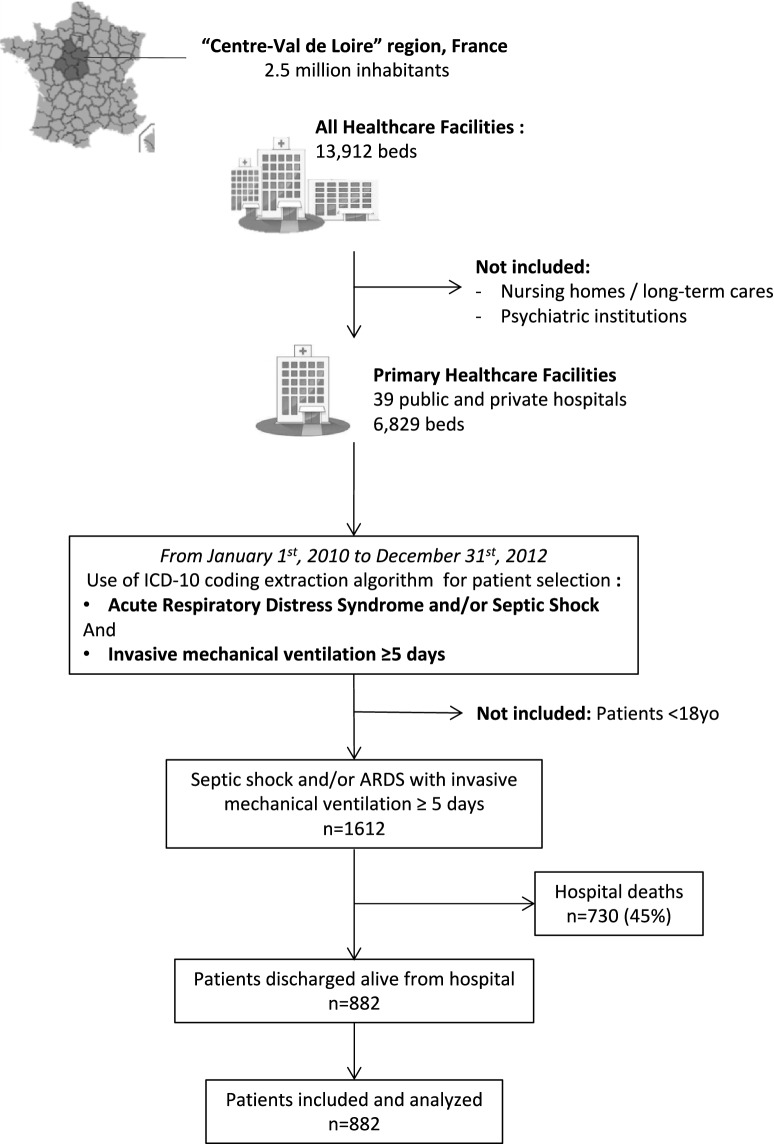
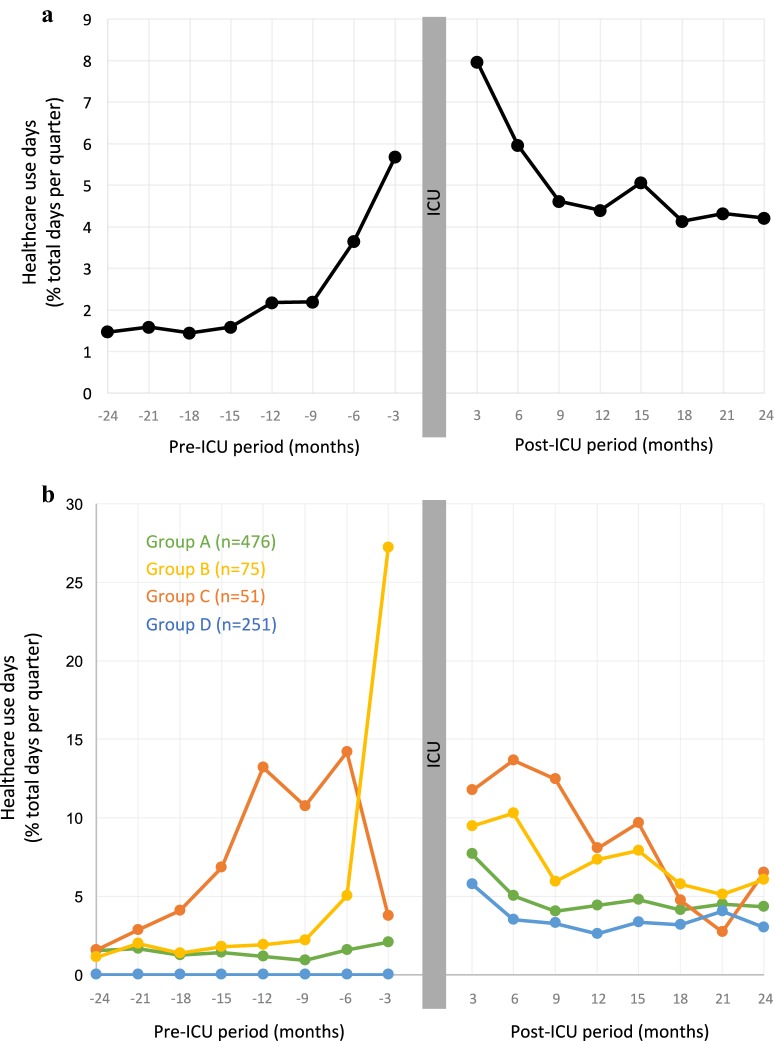
Using discharge databases in a 2.5-million-people region in France, we retrieved, over 3 years, all adult patients admitted in ICU for septic shock or acute respiratory distress syndrome (ARDS), intubated at least 5 days and discharged alive from hospital: 882 patients were included. Median duration of mechanical ventilation was 11 days (interquartile ranges [IQR] 8;20), mean SAPS2 was 49, and median hospital length of stay was 42 days (IQR 29;64). Healthcare use (days spent in healthcare facilities) was analyzed 2 years before and 2 years after ICU admission. Prior to ICU admission, we observed, at the scale of the whole study population, a progressive increase in healthcare use. Healthcare trajectories were then explored at individual level, and patients were assembled according to their individual pre-ICU healthcare use trajectory by clusterization with the K-Means method. Interestingly, this revealed diverse trajectories, identifying patients with elevated and increasing healthcare use (n = 126), and two main groups with low (n = 476) or no (n = 251) pre-ICU healthcare use. In ICU, however, SAPS2, duration of mechanical ventilation and length of stay were not different across the groups. Analysis of post-ICU healthcare trajectories for each group revealed that patients with low or no pre-ICU healthcare (which represented 83% of the population) switched to a persistent and elevated healthcare use during the 2 years post-ICU.
For 83% of ARDS/septic shock survivors, critical illness appears to have a pivotal role in healthcare trajectories, with a switch from a low and stable healthcare use prior to ICU to a sustained higher healthcare recourse 2 years after ICU discharge. This underpins the hypothesis of long-term critical illness and PICS-related quantifiable consequences in healthcare use, measurable at a population level.
重症监护后综合征(PICS)包含各种残疾情况,且与大量医疗资源使用相关。然而,患者在重症监护病房(ICU)入院前的合并症和现存医疗状况可能在一定程度上导致了ICU出院后的医疗资源使用。为了更好地理解与先前存在的合并症相比,危重症和PICS作为危重症后医疗资源使用潜在决定因素的相对贡献,我们对患者的医疗资源使用轨迹进行了基于人群的评估。
利用法国一个拥有250万人口地区的出院数据库,我们在3年时间里检索了所有因感染性休克或急性呼吸窘迫综合征(ARDS)入住ICU、机械通气至少5天且出院存活的成年患者:共纳入882例患者。机械通气的中位持续时间为11天(四分位间距[IQR]8;20),平均简化急性生理学评分系统(SAPS2)为49,中位住院时间为42天(IQR 29;64)。对ICU入院前2年和入院后2年的医疗资源使用情况(在医疗机构花费的天数)进行了分析。在ICU入院前,我们在整个研究人群层面观察到医疗资源使用呈逐渐增加趋势。随后在个体层面探索医疗轨迹,并通过K均值法聚类,根据患者入院前的个体医疗轨迹将患者分组。有趣的是,这揭示了不同的轨迹,识别出医疗资源使用升高且持续增加的患者(n = 126),以及两个主要组,一组入院前医疗资源使用较低(n = 476),另一组入院前无医疗资源使用(n = 251)。然而,在ICU中,各组间的SAPS2、机械通气持续时间和住院时间并无差异。对每组患者ICU后的医疗轨迹分析显示,入院前医疗资源使用低或无的患者(占总体的83%)在ICU后2年转变为持续且升高的医疗资源使用。
对于83%的ARDS/感染性休克幸存者,危重症似乎在医疗轨迹中起关键作用,从ICU入院前低且稳定的医疗资源使用转变为ICU出院后2年持续更高的医疗资源需求。这支持了危重症和PICS在医疗资源使用方面存在长期可量化后果的假设,且在人群层面可测量。