Department of Respiratory and Critical Care Medicine, Beijing Chao-Yang Hospital, Capital Medical University, Beijing Institute of Respiratory Medicine, Beijing Engineering Research Center for Diagnosis and Treatment of Respiratory and Critical Care Medicine (Beijing Chao-Yang Hospital), Beijing Key Laboratory of Respiratory and Pulmonary Circulation Disorders, Beijing, China.
Department of Respiratory and Critical Care Medicine, Wuhan Pulmonary Hospital, Wuhan, China.
Chest. 2020 Jul;158(1):195-205. doi: 10.1016/j.chest.2020.03.032. Epub 2020 Mar 26.
Since the outbreak of coronavirus disease 2019 (COVID-19) in China in December 2019, considerable attention has been focused on its elucidation. However, it is also important for clinicians and epidemiologists to differentiate COVID-19 from other respiratory infectious diseases such as influenza viruses.
The aim of this study was to explore the different clinical presentations between COVID-19 and influenza A (H1N1) pneumonia in patients with ARDS.
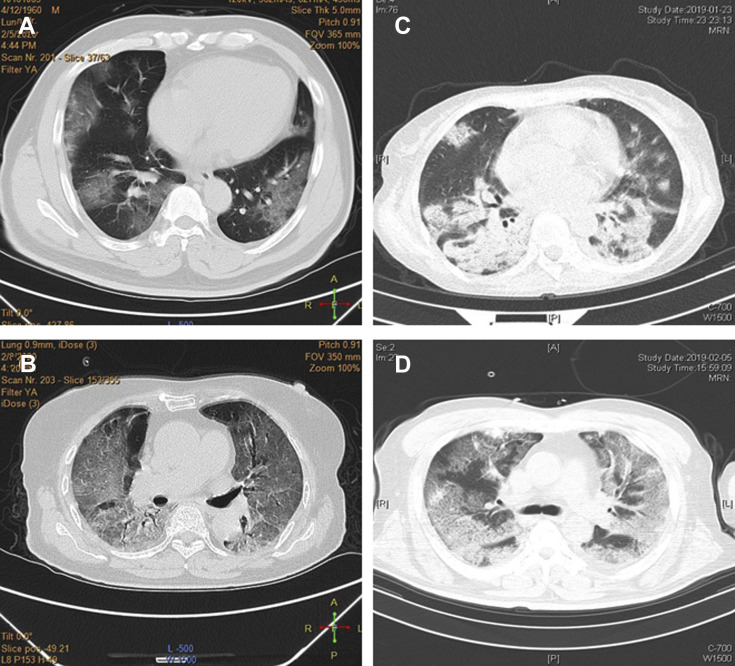
This analysis was a retrospective case-control study. Two independent cohorts of patients with ARDS infected with either COVID-19 (n = 73) or H1N1 (n = 75) were compared. Their clinical manifestations, imaging characteristics, treatments, and prognosis were analyzed and compared.
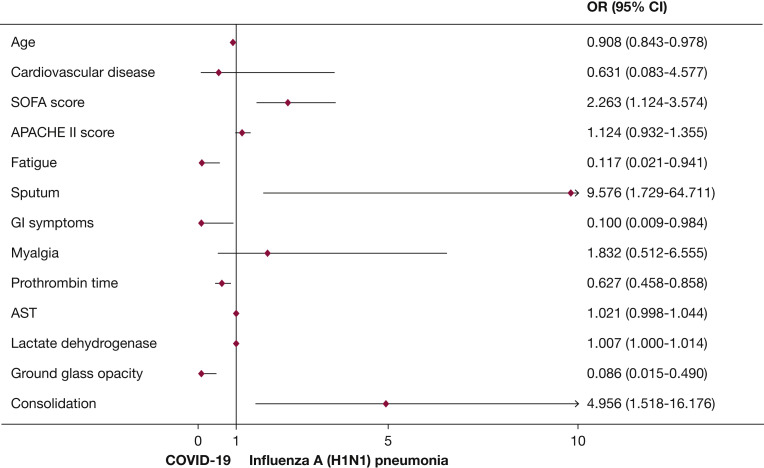
The median age of patients with COVID-19 was higher than that of patients with H1N1, and there was a higher proportion of male subjects among the H1N1 cohort (P < .05). Patients with COVID-19 exhibited higher proportions of nonproductive coughs, fatigue, and GI symptoms than those of patients with H1N1 (P < .05). Patients with H1N1 had higher Sequential Organ Failure Assessment (SOFA) scores than patients with COVID-19 (P < .05). The Pao/Fio of 198.5 mm Hg in the COVID-19 cohort was significantly higher than the Pao/Fio of 107.0 mm Hg in the H1N1 cohort (P < .001). Ground-glass opacities was more common in patients with COVID-19 than in patients with H1N1 (P < .001). There was a greater variety of antiviral therapies administered to COVID-19 patients than to H1N1 patients. The in-hospital mortality of patients with COVID-19 was 28.8%, whereas that of patients with H1N1 was 34.7% (P = .483). SOFA score-adjusted mortality of H1N1 patients was significantly higher than that of COVID-19 patients, with a rate ratio of 2.009 (95% CI, 1.563-2.583; P < .001).
There were many differences in clinical presentations between patients with ARDS infected with either COVID-19 or H1N1. Compared with H1N1 patients, patients with COVID-19-induced ARDS had lower severity of illness scores at presentation and lower SOFA score-adjusted mortality.
自 2019 年 12 月中国爆发新冠肺炎(COVID-19)以来,人们对其进行了大量研究。然而,临床医生和流行病学家区分 COVID-19 与流感病毒等其他呼吸道传染病也很重要。
本研究旨在探讨 ARDS 患者中 COVID-19 与甲型流感(H1N1)肺炎的不同临床表现。
本分析为回顾性病例对照研究。比较了两组 ARDS 患者,一组感染 COVID-19(n=73),另一组感染 H1N1(n=75)。分析并比较了他们的临床表现、影像学特征、治疗和预后。
COVID-19 患者的中位年龄高于 H1N1 患者,H1N1 组男性比例较高(P<.05)。COVID-19 患者较 H1N1 患者更易出现无痰咳嗽、乏力和胃肠道症状(P<.05)。H1N1 患者的序贯器官衰竭评估(SOFA)评分高于 COVID-19 患者(P<.05)。COVID-19 组的 PaO2/FIO2 为 198.5mmHg,明显高于 H1N1 组的 107.0mmHg(P<.001)。COVID-19 患者更常见磨玻璃影(P<.001)。COVID-19 患者接受的抗病毒治疗种类多于 H1N1 患者。COVID-19 患者的住院死亡率为 28.8%,H1N1 患者为 34.7%(P=.483)。SOFA 评分校正后的 H1N1 患者死亡率明显高于 COVID-19 患者,率比为 2.009(95%可信区间,1.563-2.583;P<.001)。
ARDS 患者感染 COVID-19 或 H1N1 时,临床表现存在许多差异。与 H1N1 患者相比,COVID-19 诱导的 ARDS 患者的疾病严重程度评分较低,SOFA 评分校正后的死亡率较低。