Department of Oncology, Copenhagen University Hospital, Copenhagen, Section 5073, Rigshospitalet, Blegdamsvej 9, 2100, Copenhagen, Denmark.
Centre for Research Ethics & Bioethics, Uppsala University, Box 564, 751 22, Uppsala, Sweden.
BMC Cancer. 2020 May 8;20(1):401. doi: 10.1186/s12885-020-06916-z.
Research and cancer care are closely intertwined; however, it is not clear whether physicians and nurses believe that clinical trials offer the best treatment for patients and, if so, whether this belief is justified. The aim of this study was therefore: (i) to explore how physicians and nurses perceive the benefits of clinical trial participation compared with standard care and (ii) whether it is justified to claim that clinical trial participation improves outcomes for cancer patients.
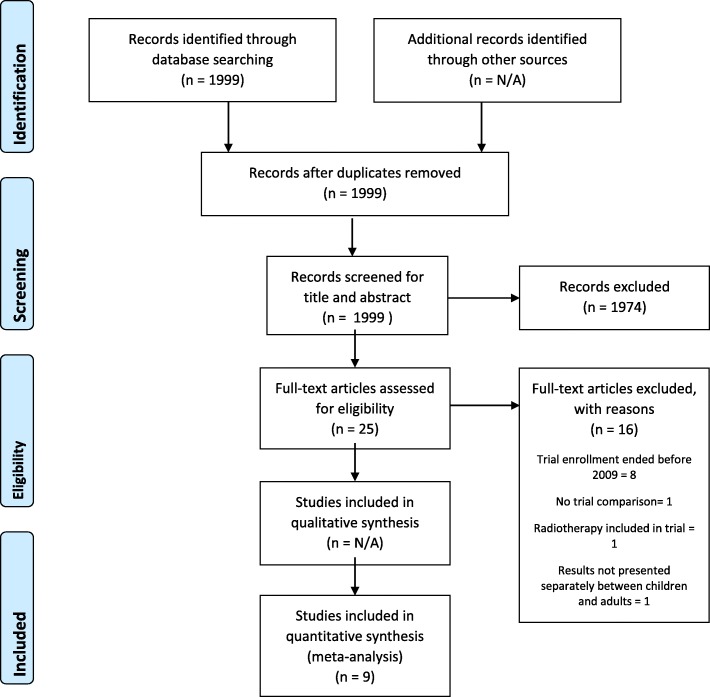
A mixed methods approach was used employing semi-structured interviews with 57 physicians and nurses in oncology and haematology and a literature review of the evidence for trial superiority, i.e. the idea that receiving treatment in a clinical trial leads to a better outcome compared with standard care. Inductive thematic analysis was used to examine the interview data. A literature review comprising nine articles was conducted according to a conceptual framework developed by Peppercorn et al. and evaluated recent evidence on trial superiority.
Our findings show that many physicians and nurses make claims supporting trial superiority, however very little evidence is available in the literature comparing outcomes for trial participants and non-participants that supports their assertions.
Despite the recent rapid development and use of targeted therapy and immunotherapy, we find no support for trial participation to provide better outcomes for cancer patients than standard care. Hence, our present results are in line with previous results from Peppercorn et al. A weaker version of the superiority claim is that even if a trial does not bring about a direct positive effect, it brings about indirect positive effects. However, as the value of such indirect effects is dependent on the individual's specific circumstances and preferences, their existence cannot establish the general claim that treatment in trials is superior. Belief in trial superiority is therefore unfounded. Hence, if such beliefs are communicated to patients in a trial recruitment context, it would provide misleading information. Instead emphasis should be on patients volunteering to give an altruistic contribution to the furthering of knowledge and to the potential benefit of future patients.
研究和癌症护理密切相关;然而,目前尚不清楚医生和护士是否认为临床试验为患者提供了最佳治疗方法,如果是这样,这种信念是否合理。因此,本研究的目的是:(i)探讨医生和护士如何看待临床试验参与相对于标准护理的益处;(ii)是否有理由声称临床试验参与改善了癌症患者的结局。
采用混合方法,对肿瘤学和血液学的 57 名医生和护士进行半结构化访谈,并对试验优越性的证据进行文献回顾,即接受临床试验治疗比标准护理的结果更好的观点。采用归纳主题分析方法对访谈数据进行分析。根据 Peppercorn 等人提出的概念框架,进行了包括 9 篇文章的文献综述,并评估了最近关于试验优越性的证据。
我们的研究结果表明,许多医生和护士都提出了支持试验优越性的主张,但文献中几乎没有比较试验参与者和非参与者的结果来支持他们的主张的证据。
尽管最近靶向治疗和免疫治疗的快速发展和应用,我们没有发现临床试验比标准护理为癌症患者提供更好结局的支持。因此,我们目前的结果与 Peppercorn 等人之前的结果一致。试验优越性的一个较弱版本是,即使试验没有直接产生积极效果,它也会产生间接的积极效果。然而,由于这种间接效果的价值取决于个人的具体情况和偏好,因此它们的存在并不能证明试验治疗优越的一般主张。因此,对试验优越性的信念是没有根据的。因此,如果在试验招募背景下向患者传达这种信念,将会提供误导性信息。相反,应该强调患者自愿为知识的进一步发展和未来患者的潜在利益做出利他贡献。