Kysthospitalet in Hagevik, Orthopedic Clinic, Haukeland University Hospital, Bergen, Norway.
Department of Clinical Medicine, University of Bergen, Bergen, Norway.
JAMA Netw Open. 2020 Sep 1;3(9):e2015015. doi: 10.1001/jamanetworkopen.2020.15015.
Conflicting evidence and large practice variation are present in the surgical treatment of degenerative spondylolisthesis. More than 90% of surgical procedures in the United States include instrumented fusion compared with 50% or less in other countries.
To evaluate whether the effectiveness of microdecompression alone is noninferior to decompression with instrumented fusion in a real-world setting.
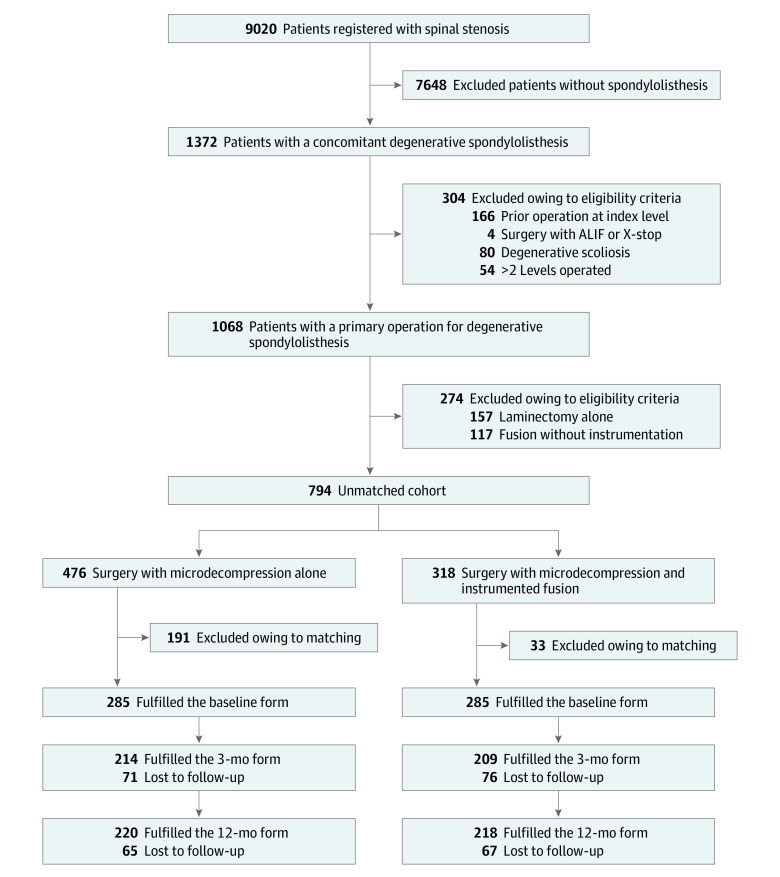
DESIGN, SETTING, AND PARTICIPANTS: This multicenter comparative effectiveness study with a noninferiority design assessed prospective data from the Norwegian Registry for Spine Surgery. From September 19, 2007, to December 21, 2015, 1376 patients at 35 Norwegian orthopedic and neurosurgical departments underwent surgery for lumbar spinal stenosis with degenerative spondylolisthesis without scoliosis. After excluding patients undergoing laminectomy alone, fusion without instrumentation, or surgery in more than 2 levels and those with a former operation at the index level, 794 patients were included in the analyses, regardless of missing or incomplete follow-up data, before propensity score matching. Data were analyzed from March 20 to October 30, 2018.
Microdecompression alone or decompression with instrumented fusion.
A reduction from baseline of 30% or greater in the Oswestry Disability Index at 12-month follow-up.
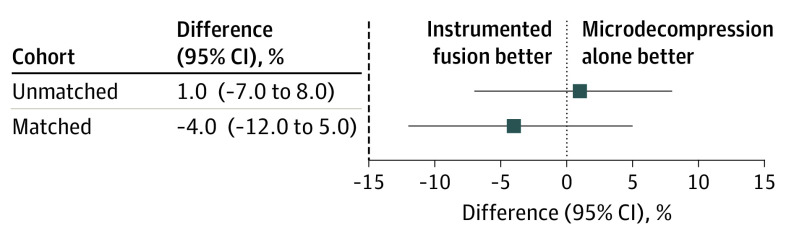
After propensity score matching, 570 patients (413 female [72%]; mean [SD] age, 64.7 [9.5] years) were included for comparison, with 285 undergoing microdecompression (mean [SD] age, 64.6 [9.8] years; 205 female [72%]) and 285 undergoing decompression with instrumented fusion (mean [SD] age, 64.8 [9.2] years; 208 female [73%]). The proportion of each type of procedure varied between departments. However, changes in outcome scores varied within patients but not between departments. The proportion of patients with improvement in the Oswestry Disability Index of at least 30% was 150 of 219 (68%) in the microdecompression group and 155 of 215 (72%) in the instrumentation group. The 95% CI (-12% to 5%) for the difference of -4% was above the predefined margin of noninferiority (-15%). Microdecompression alone was associated with shorter operation time (mean [SD], 89 [44] vs 180 [65] minutes; P < .001) and shorter hospital stay (mean [SD], 2.5 [2.4] vs 6.4 [3.0] days; P < .001).
Among patients with degenerative spondylolisthesis, the clinical effectiveness of microdecompression alone was noninferior to that of decompression with instrumented fusion. Microdecompression alone was also associated with shorter durations of surgery and hospital stay, supporting the suggestion that the less invasive procedure should be considered for most patients.
在退行性脊椎滑脱的手术治疗中,存在相互矛盾的证据和大量的实践差异。与其他国家相比,美国超过 90%的手术包括器械融合,而其他国家的比例为 50%或更低。
评估在真实环境中单纯减压与减压加器械融合的有效性是否无差异。
设计、地点和参与者:这项多中心比较有效性研究采用非劣效性设计,评估了挪威脊柱外科登记处的前瞻性数据。从 2007 年 9 月 19 日至 2015 年 12 月 21 日,35 个挪威骨科和神经外科部门的 1376 名患者因无脊柱侧凸的腰椎管狭窄伴退行性脊椎滑脱接受了手术。在排除单纯行椎板切除术、无器械融合的融合术或 2 个以上水平的手术以及指数水平有既往手术的患者后,在进行倾向评分匹配之前,共有 794 例患者被纳入分析,无论是否存在缺失或不完整的随访数据。数据于 2018 年 3 月 20 日至 10 月 30 日进行分析。
单纯减压或减压加器械融合。
在 12 个月的随访中,Oswestry 残疾指数降低 30%或更多。
在进行倾向评分匹配后,570 例患者(413 例女性[72%];平均[SD]年龄 64.7[9.5]岁)被纳入比较,其中 285 例行单纯减压(平均[SD]年龄 64.6[9.8]岁;205 例女性[72%]),285 例行减压加器械融合(平均[SD]年龄 64.8[9.2]岁;208 例女性[73%])。不同科室的手术类型比例有所不同。然而,患者的治疗结果在变化,但不同科室之间没有变化。219 例接受单纯减压的患者中,150 例(68%)Oswestry 残疾指数改善至少 30%,215 例接受器械融合的患者中,155 例(72%)Oswestry 残疾指数改善至少 30%。差异为-4%,95%置信区间(-12%至 5%)在预定的非劣效性边界(-15%)之上。单纯减压与较短的手术时间(平均[SD],89[44]分钟比 180[65]分钟;P < .001)和较短的住院时间(平均[SD],2.5[2.4]天比 6.4[3.0]天;P < .001)相关。
在退行性脊椎滑脱患者中,单纯减压的临床效果与减压加器械融合无差异。单纯减压还与手术和住院时间较短有关,这支持了对大多数患者应考虑采用微创术式的建议。