Department of Pediatrics, Stanford University School of Medicine, Stanford, CA, USA.
Child Health Research Foundation, Dhaka, Bangladesh.
BMJ Open. 2020 Nov 4;10(11):e042380. doi: 10.1136/bmjopen-2020-042380.
Describe the pattern of atopic disease prevalence from infancy to adulthood.
Cross-sectional household survey.
Community-based demographic surveillance site, Mirzapur, Bangladesh.
7275 individuals in randomly selected clusters within 156 villages.
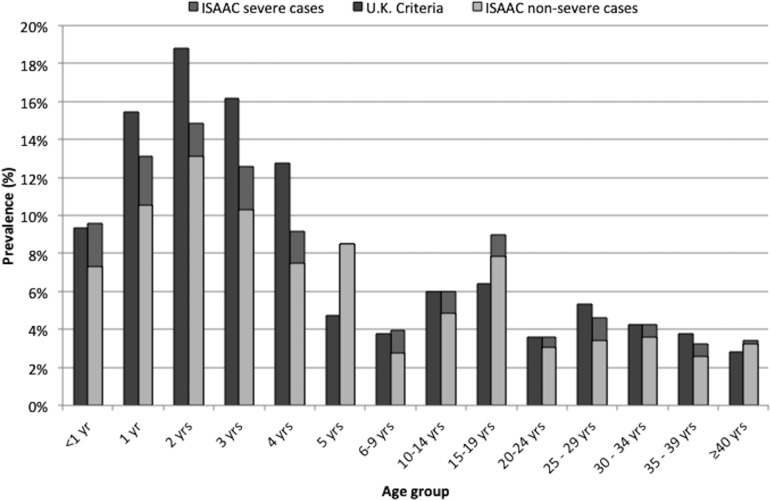
The 12-month prevalence of atopic dermatitis (by UK Working Party Criteria (UK criteria) and International Study of Asthma and Allergies in Childhood (ISAAC)), asthma and rhinitis (by ISAAC); disease severity (by ISAAC); history of ever receiving a medical diagnosis.
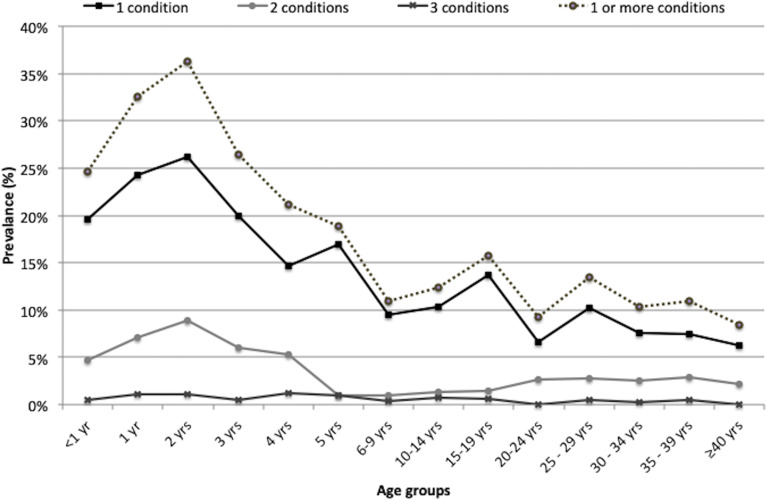
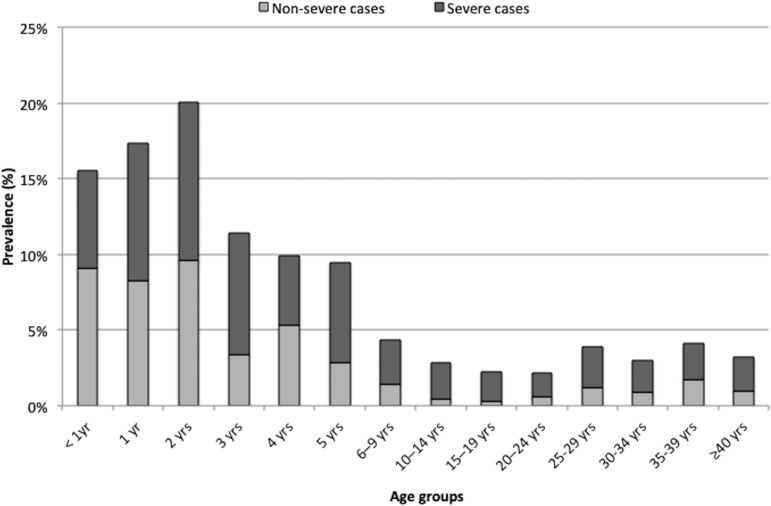
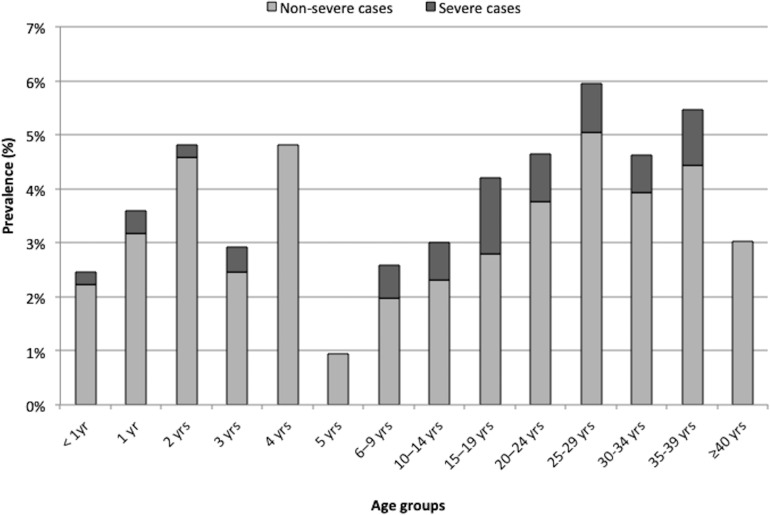
Children aged 2 years had the highest prevalence of atopic dermatitis-18.8% (95% CI 15.2% to 22.4%) by UK criteria and 14.9% (95% CI 11.6% to 18.1%) by ISAAC- and asthma (20.1%, 95% CI 16.4% to 23.8%). Prevalence of rhinitis was highest among 25-29 year olds (6.0%, (95% CI% 4.5 to 7.4%). History of a medical diagnosis was lowest for atopic dermatitis (4.0%) and highest for rhinitis (27.3%) and was significantly associated with severe disease compared with those without severe disease for all three conditions (atopic dermatitis: 30.0% vs 11.7%, p=0.015; asthma; 85.0% vs 60.4%, p<0.001; rhinitis: 34.2% vs 7.3%, p<0.001) and having a higher asset-based wealth score for asthma (29.7% (highest quintile) vs 7.5% (lowest quintile), p<0.001) and rhinitis (39.8% vs 12.5%, p=0.003). Prevalence of having 1 condition was highest (36.2%) at 2 years and decreased with age. Having atopic dermatitis (ISAAC) was associated with significantly increased odds ratios (OR) for comorbid asthma (OR 5.56 (95% CI 4.26 to 7.26)] and rhinitis (3.68 (95% CI 2.73 to 4.96)). Asthma and rhinitis were also strongly associated with each other (OR 8.39 (95% CI 6.48 to 10.86)).
Atopic disease burden was high in this rural Bangladeshi population. Having one atopic condition was significantly associated with the presence of another. Low incidence of ever obtaining a medical diagnosis highlights an important opportunity to increase availability of affordable diagnosis and treatment options for all age groups.
描述从婴儿期到成年期特应性疾病的流行模式。
横断面家庭调查。
孟加拉国米尔扎布尔社区为基础的人口监测点。
随机选择的 156 个村庄内的 7275 名个体。
特应性皮炎(按英国工作组标准(英国标准)和儿童国际哮喘和过敏研究(ISAAC))、哮喘和鼻炎(按 ISAAC)的 12 个月患病率;疾病严重程度(按 ISAAC);既往接受过医疗诊断的情况。
2 岁儿童特应性皮炎的患病率最高-英国标准为 18.8%(95%CI 15.2%至 22.4%),ISAAC 为 14.9%(95%CI 11.6%至 18.1%);哮喘(20.1%,95%CI 16.4%至 23.8%)。25-29 岁人群鼻炎患病率最高(6.0%,95%CI%为 4.5%至 7.4%)。有医疗诊断史的特应性皮炎(4.0%)和鼻炎(27.3%)最低,与所有三种疾病的无严重疾病者相比,严重疾病的发生率显著更高(特应性皮炎:30.0% vs 11.7%,p=0.015;哮喘;85.0% vs 60.4%,p<0.001;鼻炎:34.2% vs 7.3%,p<0.001),并且哮喘(29.7%(最高五分位数)vs 7.5%(最低五分位数),p<0.001)和鼻炎(39.8% vs 12.5%,p=0.003)的资产基础财富评分较高。患有 1 种疾病的患病率最高(36.2%)在 2 岁时,随着年龄的增长而降低。患有特应性皮炎(ISAAC)与合并哮喘(OR 5.56(95%CI 4.26 至 7.26))和鼻炎(OR 3.68(95%CI 2.73 至 4.96))的相关优势比显著增加。哮喘和鼻炎之间也存在很强的相关性(OR 8.39(95%CI 6.48 至 10.86))。
在这个孟加拉国农村地区,特应性疾病负担很高。患有一种特应性疾病与另一种疾病的存在显著相关。既往获得医疗诊断的发病率低,这为增加所有年龄段人群获得负担得起的诊断和治疗选择提供了重要机会。