Department of Orthopedics, The Second Hospital of Tianjin Medical University, Tianjin, China.
Department of Orthopedics Emergency, Tianjin Hospital, Tianjin, China.
Orthop Surg. 2021 Jun;13(4):1149-1158. doi: 10.1111/os.12906. Epub 2021 May 4.
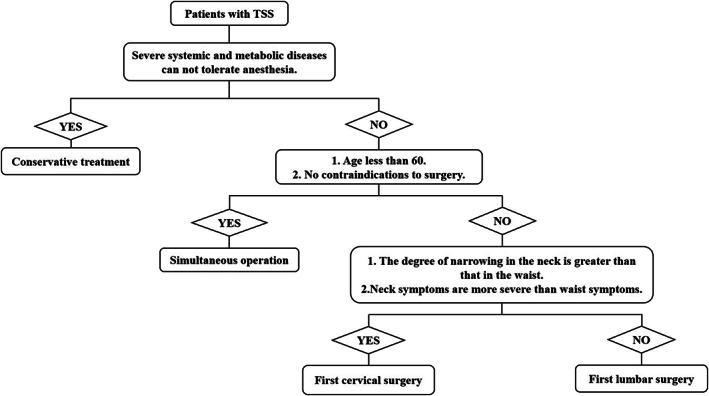
To compare the clinical effects of cervical decompression first, lumbar decompression first, or simultaneous decompression of both lesions in the treatment of tandem spinal stenosis (TSS).
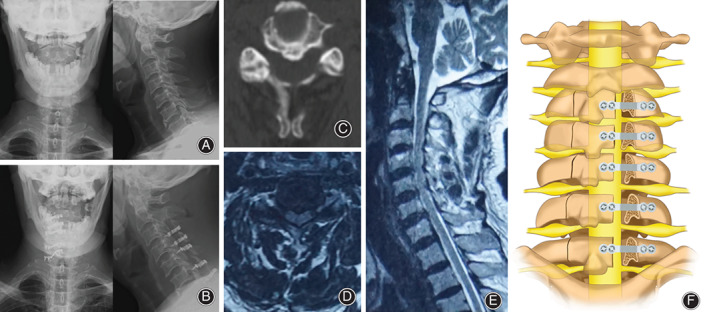
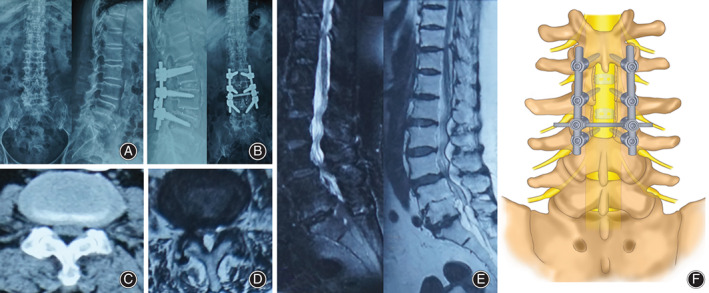
This is a retrospective analysis. From January 2013 to December 2018, 51 TSS patients underwent our surgery and postoperative investigation. Among the 51 subjects, 27 females and 24 males, aged 49-77 years with an average age of 66.3 ± 6.8, were selected. According to the different operation sequences, all patients were divided into three groups. In simultaneous operation group, five patients underwent cervical and lumbar vertebrae surgery at the same time. In first cervical surgery group, 28 patients underwent cervical vertebra surgery first, followed by lumbar spine surgery after a period of recovery. And in first lumbar surgery group, 18 patients underwent lumbar vertebrae surgery first. The choice for neck surgery is posterior cervical single-door vertebroplasty, the surgery of lumber is plate excision and decompression needle-rod system internal fixation. The outcome measures are visual analogue scale (VAS), Japanese Orthopaedic Association cervical (JOA-C) and lumbar (JOA-L) scores, which were assessed at 3 months and 1 year after the operation by telephone interview. In addition, operative time, estimated blood loss, and hospital stay were also recorded.
All the patients in the study had surgery performed successfully by the same group of orthopaedic surgeons. The preoperative VAS scores of simultaneous operation group, first cervical surgery group, and first lumbar surgery group were 8.00 ± 1.00, 8.36 ± 0.68, and 8.17 ± 0.71 (P > 0.05). The preoperative JOA-C scores were 7.00 ± 2.35, 6.54 ± 1.53, and 7.83 ± 1.04 (P < 0.05). And the preoperative JOA-L scores were 7.20 ± 2.17, 4.64 ± 2.36, and 5.78 ± 1.22 respectively (P < 0.05). During the final 1-year follow-up, the JOA-C improvement rates of simultaneous operation group, first cervical surgery group, and first lumbar surgery group were 85.68% ± 5.44%, 84.27% ± 5.02%, and 83.34% ± 10.25%, respectively (P > 0.05), and the JOA-L improvement rates were 80.04% ± 3.35%, 81.65% ± 3.74%, and 80.21% ± 4.76% (P > 0.05). The difference among them was not statistically significant. In addition, operation time (OP), blood loss (BL), and hospital stay (HS) in the simultaneous operation group were 245.00 ± 5.00 min, 480.00 ± 27.39 mL, and 16.60 ± 0.55 days, respectively. While those parameters in the first cervical surgery group were 342.50 ± 18.18 min, 528.21 ± 43.97 mL, and 22.75 ± 2.15 days, and in the first lumbar surgery group they were 346.11 ± 24.77 min, 519.44 ± 43.99 mL, and 22.89 ± 1.64 days. The average blood loss in simultaneous operation group was less (P > 0.05); meanwhile, the operation time and hospital stay time were significantly shorter in the simultaneous operation group than in the first cervical surgery group and first lumbar surgery group (P < 0.05). Only one case of fat liquefaction occurred in first cervical surgery group, which healed spontaneously after a regular change of dressing for 1 month.
Under the condition of ensuring the surgical effect, the choice of staged surgery or concurrent surgery according to the patients' own symptoms of cervical and lumbar symptoms could both obtain satisfactory results, and the damage of simultaneous surgery was less than that of staged surgery.
比较颈椎减压优先、腰椎减压优先与颈椎、腰椎同时减压治疗串联性脊柱狭窄(TSS)的临床效果。
这是一项回顾性分析。2013 年 1 月至 2018 年 12 月,51 例 TSS 患者接受了我们的手术和术后调查。51 例患者中,女性 27 例,男性 24 例,年龄 49-77 岁,平均年龄 66.3±6.8 岁。根据不同的手术顺序,所有患者分为三组。在同期手术组中,5 例患者同时进行颈椎和腰椎手术。在颈椎手术组中,28 例患者首先进行颈椎手术,恢复一段时间后再进行腰椎手术。在腰椎手术组中,18 例患者首先进行腰椎手术。颈椎手术选择后路颈椎单开门椎体成形术,腰椎手术采用板切除减压针棒系统内固定。通过电话访谈,在术后 3 个月和 1 年评估视觉模拟量表(VAS)、日本骨科协会颈椎(JOA-C)和腰椎(JOA-L)评分。此外,还记录了手术时间、估计失血量和住院时间。
所有患者均由同组骨科医生成功完成手术。同期手术组、颈椎手术组和腰椎手术组的术前 VAS 评分分别为 8.00±1.00、8.36±0.68 和 8.17±0.71(P>0.05)。术前 JOA-C 评分分别为 7.00±2.35、6.54±1.53 和 7.83±1.04(P<0.05)。术前 JOA-L 评分分别为 7.20±2.17、4.64±2.36 和 5.78±1.22(P<0.05)。在最终 1 年随访中,同期手术组、颈椎手术组和腰椎手术组的 JOA-C 改善率分别为 85.68%±5.44%、84.27%±5.02%和 83.34%±10.25%(P>0.05),JOA-L 改善率分别为 80.04%±3.35%、81.65%±3.74%和 80.21%±4.76%(P>0.05)。它们之间的差异没有统计学意义。此外,同期手术组的手术时间(OP)、失血量(BL)和住院时间(HS)分别为 245.00±5.00min、480.00±27.39mL 和 16.60±0.55d,而颈椎手术组分别为 342.50±18.18min、528.21±43.97mL 和 22.75±2.15d,腰椎手术组分别为 346.11±24.77min、519.44±43.99mL 和 22.89±1.64d。同期手术组的平均失血量较少(P>0.05);同时,同期手术组的手术时间和住院时间明显短于颈椎手术组和腰椎手术组(P<0.05)。颈椎手术组仅 1 例发生脂肪液化,经 1 个月常规换药后自行愈合。
在保证手术效果的前提下,根据患者自身颈椎和腰椎症状的特点,选择分期手术或同期手术均可获得满意的效果,同期手术的损伤小于分期手术。